MEDICAL: DISEASES: ZIKA VIRUS :
GUIDES :
DIRECTORIES :
PUBLICATIONS :
MEDICAL: RESOURCES:
Zika Virus for Healthcare Providers
FROM Centers for Disease Control and Prevention.
National Center for Emerging and Zoonotic Infectious Diseases (NCEZID).
Division of Vector-Borne Diseases (DVBD) PART TWO
http://www.cdc.gov/zika/index.html
Contents of the Posts for These Documents
CDCZika Virus HomeMosquito Control
Potential Range in US
Language:
English
Recommend on FacebookTweet
Estimated range of Aedes albopictus and Aedes aegypti in the United States, 2016*
*Maps have been updated from a variety of sources. These maps represent CDC’s best estimate of the potential range of Aedes aegypti and Aedes albopictus in the United States. Maps are not meant to represent risk for spread of disease.
Estimated range of Aedes albopictus and Aedes aegypti in the United States, 2016 Maps[PDF – 1 page]
The new estimated range maps have been updated from a variety of published and unpublished sources. These maps show CDC’s best estimate of the potential range of Aedes aegypti and Aedes albopictus in the United States. These maps include areas where mosquitoes are or have been previously found. Maps are not meant to represent risk for spread of disease. Aedes aegypti mosquitoes are more likely to spread viruses like Zika, dengue, chikungunya and other viruses than other types of mosquitoes such as Aedes albopictus mosquitoes
These maps show
- The new estimated range maps have been updated from a variety of published and unpublished sources.
- These maps show CDC’s best estimate of the potential range of Aedes aegypti andAedes albopictus in the United States.
- These maps include areas where mosquitoes are or have been previously found.
- Maps are not meant to represent risk for spread of disease.
These maps DO NOT show
- Likelihood that these mosquitoes will spread viruses. Shaded areas on the map do not necessarily mean that there are infected mosquitoes in that area.
- Numbers of mosquitoes: These maps do not show how many mosquitoes are living in an area. Mosquito population numbers vary widely across the shaded areas on the map, from high numbers of mosquitoes in some parts of Florida and Texas to rare reports of mosquitoes further north.
- Exact locations of mosquitoes: These maps are our best estimate of where mosquitoes could potentially live. Actual mosquito populations will vary by state and county. Mosquito populations may be found in an area that is not shaded on the maps and may not be found in all shaded areas.
About these mosquitoes
Aedes aegypti
- These mosquitoes live in tropical, subtropical, and in some temperate climates.
- They are the main type of mosquito that spread Zika, dengue, chikungunya, and other viruses.
- Because Aedes aegypti mosquitoes live near and prefer to feed on people, they are more likely to spread these viruses than other types of mosquitoes.
Aedes albopictus
- These mosquitoes live tropical, subtropical, and temperate climates, but can live in a broader temperature range and at cooler temperatures than Aedes aegypti.
- Because these mosquitoes feed on animals as well as people, they are less likely to spread viruses like Zika, dengue, chikungunya and other viruses.
About outbreaks spread by mosquitoes
- Local mosquito-borne Zika virus transmission has been reported in the continental United States.
- Many areas in the United States have the type of mosquitoes that can become infected with and spread Zika, chikungunya, and dengue viruses.
- Recent outbreaks in the continental United States of chikungunya and dengue, which are spread by the same type of mosquito, have been relatively small and limited to a small area.
- Areas with past outbreaks of chikungunya and dengue are considered at higher risk for Zika. These include U.S. territories like Puerto Rico, the U.S. Virgin Islands, and Guam. Local outbreaks have also been reported in parts of Hawaii, Florida, and Texas.
- Aedes aegypti or Aedes albopictus mosquitoes can cause an outbreak, if all of the following happens:
- People get infected with a virus (like Zika, dengue, or chikungunya).
- An Aedes aegypti or Aedes albopictus mosquito bites an infected person during the first week of infection when the virus can be found in the person’s blood.
- The infected mosquito lives long enough for the virus to multiply and for the mosquito to bite another person.
- The cycle continues multiple times to start an outbreak.
Protect yourself from Zika and other viruses spread by mosquitoes
- The best way to prevent Zika and other viruses spread through mosquito bites is to take steps to prevent mosquito bites[PDF – 2 pages]. If you are pregnant, strictly follow these steps:
- Wear long-sleeved shirts and long pants.
- Stay in places with air conditioning and use window and door screens to keep mosquitoes outside.
- Use Environmental Protection Agency (EPA)-registered insect repellents with one of the following active ingredients: DEET, picaridin, IR3535, oil of lemon eucalyptus, or para-menthane-diol. When used as directed, EPA-registered insect repellents are proven safe and effective, even for pregnant and breastfeeding women.
- Treat clothing with permethrin or purchase permethrin-treated items.
For more information about how to prevent mosquito bites, see Mosquito Bite Prevention (United States)[PDF – 2 pages].
For Professionals
Language:
English
Recommend on FacebookTweet
In the continental United States, vector control professionals use integrated vector management strategies to control Aedes aegypti and Aedes albopictus mosquitoes.
- Before a locally-acquired case(s) of Zika, chikungunya, or dengue virus infection occurs, professionals conduct surveillance to understand local populations of mosquitoes and begin control efforts.
- If a travel-related case is reported or locally-acquired case is suspected, vector control professionals enhance mosquito control activities to reduce both larvae and adult mosquito densities. This can help keep mosquitoes from biting infected people, which can break the transmission cycle.
- Vector surveillance and control efforts should target mosquito species that can transmit viruses. Control activities are generally similar for both Aedes aegypti andAedes albopictus mosquitoes.
SURVEILLANCE & CONTROL
INSECTICIDE RESISTANCE
DISINSECTION
For ELC Recipients
CDC’s Epidemiology & Laboratory Capacity for Infectious Diseases (ELC) Cooperative Agreement funds have been distributed to develop or enhance mosquito vector surveillance and insecticide resistance testing and to report results to CDC. Data compiled from ELC recipients will be used to develop more accurate knowledge of where and during what time of the year Zika virus mosquito vectors (Aedes aegypti and Aedes albopictus) occur in the United States, and when and where these mosquitoes are most abundant. Additionally, data will be used to track insecticide resistance in Zika virus mosquito vectors across space and time throughout the United States.
In order to facilitate data collection and reporting, download the following documents.
Photos courtesy of Ed Freytag, City of New Orleans Mosquito & Termite Control Board
Surveillance and Control of Aedes aegypti and Aedes albopictus in the United States
Language:
English
Recommend on FacebookTweet
Surveillance of Aedes aegypti and Aedes albopictus
Intended audience: ELC recipients conducting mosquito surveillance and insecticide resistance testing
Control of Aedes aegypti and Aedes albopictus
Intended audience: Vector control professionals
Disinsection
Language:
English
Recommend on FacebookTweet
Technical Statement on the Role of Disinsection of Airplanes or Ships in the Context of Zika Outbreaks, 2016
Key Points
- CDC does not recommend routine use of insecticides (disinsection) inside commercial passenger airplanes or on ships to prevent the spread of Zika virus.
- An infected person is the most common source for imported mosquito-borne viruses with a human-mosquito-human transmission cycle.1
- Public health interventions for travelers should focus on preventing mosquito bites while in areas with Zika virus outbreaks and on return from those areas (for 3 weeks following return).
- Routine, established efforts to control or eliminate mosquitoes in and around airports and seaports should be followed.
Use of Disinsection in Airplanes to Control the Spread of Zika Virus
- The World Health Organization (WHO) convened an Advisory Group on aircraft disinsection in Geneva during April 2016 to discuss the role of disinsection in the spread of Zika virus. In the context of Zika virus, WHO stated: “Effectiveness of disinsection was considered low for preventing pathogen importation, as there is a low risk of importation by mosquito vectors compared to infected travelers.” However, WHO continues to recognize a possible role for disinsection in certain circumstances and advises countries to conduct a risk assessment before instating requirements. It is therefore possible that individual countries may require disinsection of aircraft originating from countries with Zika outbreaks.2
- It is thought that the probability of any mosquito being on an airplane is low (and perhaps even lower for an infected mosquito).3
- Given the use of air conditioning and the relatively brief period for potential exposure, the risk of travelers becoming infected on board an airplane through the bite of an infected mosquito is considered to be lower than their risk of being bitten by an infected mosquito while they were in affected areas.
- There is no evidence to show that using insecticide to kill mosquitoes inside aircraft cabins is effective in preventing introduction and spread of mosquito-borne diseases.
- Given lack of efficacy, drawbacks to consider include possible adverse health effects (including allergic reactions) in crew members or passengers, damage to aircraft materials, and objections by passengers and crewmembers.4, 5 The issue of emerging resistance to insecticides among mosquito species is another factor to weigh when considering disinsection.6
- There are currently no products approved by the Environmental Protection Agency for disinsection inside an occupied aircraft cabin.7
Use of Disinsection on Ships to Control the Spread of Zika Virus
- Inspection and disinsection of cargo containers are difficult and not effective mechanisms to prevent importation of Aedes aegypti or Aedes albopictusmosquitoes or Zika virus.8
- The most common way for Aedes aegypti or Aedes albopictus species mosquitoes to travel long distances is as unhatched eggs. Disinsection with conventional insecticides will not kill the eggs, which are resistant to insecticides.
- Cargo containers are unloaded rapidly from ships and might not be opened at the port but at other locations.
- These factors decrease the effectiveness of disinsection and in many instances make it infeasible.
- Ship operators, seaports, and importers should collaborate to eliminate sources of standing water that serve as places where mosquitoes can lay eggs as part of routine operations, but this should not be considered a significant countermeasure to prevent the spread of Zika virus.
Although CDC has the authority to require disinsection under parts 70 and 71 of title 42 of the Code of Federal Regulations, disinsection is not currently required for airplanes or ships arriving at US ports of entry.9 For more information, see Questions and Answers about Disinsection and Zika for the Shipping Industry and Partners and Questions and Answers about Zika for the Airline Industry and Partners.
Humans are the Most Common Way for Zika Virus to Enter a Country
- The most common way that Zika virus enters a country is by introduction of the virus to the local mosquito population by an infected traveler.
- Mosquito-borne viruses, such as dengue, chikungunya, and Zika, spread internationally primarily through infected people. This can occur when an infected person goes to a different country and is bitten by uninfected mosquitoes that then become infected. The newly infected mosquito population can then spread the virus.
- Mosquito species that can transmit the Zika virus (Aedes aegypti and Aedes albopictus) are found in many parts of the United States, so infected people arriving in the United States could be bitten in their homes or residential areas by mosquitoes, which could result in local spread.
- For these reasons, areas where these mosquitoes are located or where Zika virus is spreading should focus on local mosquito control and other prevention efforts, such as encouraging returning travelers to take measures to prevent mosquito bites.
Summary
CDC does not recommend disinsection inside commercial passenger aircraft or on ships as an effective approach to control the movement of Zika virus over long distances, such as from one country to another. CDC recommends that other local public health interventions should be the primary focus to prevent local transmission of Zika virus.
References
- SM Ostroff. The Role of the Traveler in Translocation of Disease. CDC Health Information for International Travel, 2016 Yellow Book.
- WHO Ad-hoc Advisory Group on aircraft disinsection for controlling the international spread of vector-borne diseases, Geneva, Switzerland, 21 to 22 April 2016.
- L Mier-y-Teran-Romero, AJ Tatem, and MA Johansson. Introduction of mosquito-borne diseases into non-endemic locations: infected human travelers versus mosquitoes. International Conference on Emerging Infectious Diseases[PDF – 300 pages]. August, 2015. Atlanta, Georgia, p. 261.
- CDC NIOSH. Aircrew Safety & Health. Pesticides – What you need to know.
- Advisory Group for Aerospace Research & Development. Aircraft disinsection: A guide for military & civilian air carriers. 1996.
- N Liu. Insecticide resistance in mosquitoes: Impact, mechanisms, and research directions. Annual Review of Entomology. Vol. 60: 537-559 (Volume publication date January 2015) DOI: 10.1146/annurev-ento-010814-020828
- EPA PRN 96-3: Pesticide products used to disinsect aircraft. 1996.
- EU SHIPSAN ACT. Interim guidance on maritime transport and Zika virus disease.[PDF – 20 pages] 2016.
- Code of Federal Regulations; Title 42 Public Health; parts 70 and 71.
Information on Aerial Spraying
Language:
English
Recommend on FacebookTweet
When people in a large area are getting sick or when large numbers of mosquitoes are found, airplanes can be used to treat very large areas with insecticides safely, quickly, and efficiently. This process is called aerial spraying. Below is more information on aerial spraying.
Integrated Vector Management
Is aerial spraying an effective tool for killing mosquitoes?
Aerial treatment of areas with products that rapidly reduce both young and adult mosquitoes can help to limit the number of mosquitoes that carry the Zika virus. Repeated aerial applications of insecticide has reduced mosquito populations as a part of an integrated vector management program.
Is aerial spraying alone the best way to control mosquitoes?
- Aerial spraying is only one part of the solution for controlling mosquitoes, but it is the one method that can rapidly reduce the number of mosquitoes spreading Zika in a large area.
- It is the most effective method when large areas must be treated quickly.
- Aerial spraying is used as part of an integrated mosquito control program to quickly reduce the number of mosquitoes responsible for infecting people with viruses like Zika, dengue, or chikungunya.
- An integrated mosquito control program includes
- Source reduction. Eliminating mosquito habitats, such as discarded containers and rain gutters.
- Structural barriers, such as screens and enclosed, air-conditioned spaces, if possible.
- Larval mosquito control using the appropriate methods for the habitat.
- Adult mosquito control using insecticides.
- Community education efforts related to preventing mosquito bites by wearing EPA-registered insect repellents and protective clothing (long-sleeved shirts and long pants).
Aerial Spraying and Insecticides
Is aerial spraying experimental?
- Aerial spraying is not experimental.
- EPA-registered insecticides are used for aerial spraying EPA-registered insecticides have been studied for their effectiveness and safety when used according to label instructions.
- Aerial spraying, using Naled and other insecticides, has been used in many populated areas of the continental United States, including Miami, Tampa, and New Orleans, to help control mosquitoes.
- In 2014, almost 6 million acres of land in Florida was aerial sprayed with Naled by mosquito control programs.
Where has Naled been used?
- Naled has been extensively used since the 1950s and is currently applied by aerial and ground spraying to an average of approximately 16 million acres of the continental United States annually.
- It is also used for mosquito control following natural disasters, such as hurricanes and floods. (Human Exposure to Mosquito-Control Pesticides ― Mississippi, North Carolina, and Virginia, 2002 and 2003, CDC, 2005)
- In 2004 and 2005, it was used as part of the emergency responses to Hurricanes Charley, Jeanne, Frances, and Katrina.
- Naled is currently used in the United States by many local governments and mosquito control districts, including the Florida Keys Mosquito Control District, the Lee County Mosquito Control District, and Miami-Dade County.
- Historically, Naled has been used in Puerto Rico in attempts to control dengue.
What happens to Naled once it is sprayed?
- Naled starts to degrade (break down) immediately on surfaces, in water, and in sunlight.
- The chemical dichlorvos (DDVP) can be created when Naled degrades. It also breaks down quickly.
- In small quantities DDVP has not been shown to cause health problems in people.
- DDVP does not build up in breast milk or breast tissue.
What is Bti and how does it work?
- Bacillus thuringiensis subspecies israelensis (Bti) is a naturally occurring bacteria found in soils.
- Bti produces toxins that kill the larvae of mosquitoes and blackflies when swallowed. The toxins cause death by starvation and only begin working when swallowed by certain insects (larvae of mosquitoes, blackflies, and fungus gnats).
- There are several strains of Bacillus thuringiensis (Bt) that kill other insect larva like caterpillars and beetles. These are not the same as Bti.
Can Bti only be applied through aerial spraying?
- No, Bti is often applied using methods that are not aerial spraying.
- Bti can be applied using truck-mounted or backpack spraying. It can also be found as dunks or briquettes that can be put in areas of standing water that cannot be emptied, such as fountains and ornamental ponds, septic tanks, and unchlorinated pools.
- Dunks are currently being distributed in Zika prevention kits.
Aerial Spraying and Human Health
Is aerial spraying of insecticides dangerous/harmful to human health?
- No, during aerial spraying, a small amount of insecticide is sprayed over an area, about 1 ounce (two tablespoons) per acre or about the size of a football field.
- This small amount does not pose a health risk to people or pets in the area that is sprayed.
- When aerial spraying is done correctly, it does not cause asthma attacks.
- There is a possibility that spraying of a larvicide, like Bti, can cause eye irritation if a person is outside and looking up when spraying takes place.
- EPA-registered products are used for aerial spraying. The label instructions are followed by a licensed professional.
- If people prefer to stay inside and close windows and doors when spraying takes place they can, but it is not necessary.
Does aerial spraying cause asthma attacks?
- No, when aerial spraying is done correctly, it does not cause asthma attacks.
- When applied according to label instructions, EPA-registered insecticides do not pose a risk to human health or the environment.
- Research shows that ultra-low volume (ULV) application for mosquito control does not increase the risk of asthma for people living in treatment areas (Karpati et al. 2004, Currier et al. 2005, Duprey et al. 2008).
Will Naled cause cancer?
- No, EPA has classified Naled as Group E “Evidence of Non-carcinogenicity for Humans,” meaning that there is no evidence that it causes cancer in people.
- During aerial spraying, a small amount of insecticide is sprayed over an area, about 1 ounce (two tablespoons) per acre or about the size of a football field.
- Droplets float in the air and kill adult mosquitoes on contact.
- Naled starts to degrade (break down) immediately on surfaces, in water, and in sunlight.
- EPA conducted risk assessments for Naled and calculated risks under different exposure scenarios.
- Because of the very small amount of active ingredient released per acre of ground during aerial spraying, EPA found that for all scenarios and exposures were hundreds or thousands of times below an amount that might pose a health concern.
- In an evaluation of thousands of people who conducted agricultural spraying using many types of insecticides, including organophosphates like Naled, no increased risk of any type of cancer was found during the 7-11 years of follow up (Schinasi & Leon, 2008).
- However, at high doses, for example if the person doing the spraying is exposed to Naled directly in amounts that are well above those for normal labeled uses, Naled and other organophosphates can overstimulate the nervous system, causing nausea, dizziness, or confusion. This is why it is very important that those who actually work with Naled strictly follow label instructions.
- Severe high-dose poisoning with any organophosphate can cause convulsions, respiratory paralysis, and death.
- It is extremely unlikely that any person would come into contact with this amount of Naled when it is applied by a licensed professional according to label instructions.
Will Bti affect human health?
- Bti has not been found to pose a health risk to people or pets.
- There is a possibility that spraying larvicides, like Bti, can cause eye irritation if a person is outside when spraying takes place.
- Bti is an EPA-registered insecticide. EPA-registered insecticides have been studied for their effectiveness and safety when used according to label instructions.
- Existing residential and area-wide uses, like aerial or truck spraying, have been evaluated and found to be safe. Using Bti to kill mosquito larvae may reduce the risk of getting infected with Zika virus.
- If people prefer to stay inside when spraying takes place they can, but it is not necessary.
Aerial Spraying and Animals
Will aerial spraying hurt pets and other animals?
- No, when aerial spraying is done correctly, it does not harm animals.
- During aerial spraying, a small amount of insecticide is sprayed over an area, about 1 ounce (two tablespoons) per acre, or about the size of a football field.
- This small amount does not pose a health risk to people or pets in the area that is sprayed.
- EPA-registered products are used for aerial spraying. The label instructions are followed by a licensed professional.If people prefer to bring pets inside when spraying takes place they can, but it is not necessary.
- Aerial spraying will not harm fish or animals that live in the water. People do not need to cover fish ponds when spraying takes place. If a larvicide is sprayed, it is better if ponds are not covered.
Will aerial spraying kill bees?
- Aerial spraying can be done in ways that minimize risk to bees.
- Spraying Naled can kill bees outside of their hives at the time of spraying; therefore, spraying is limited to dawn or dusk when bees are inside their hives.
- Because Naled breaks down quickly, it does not pose a risk to the honey bee populations.
- Studies show that honey production between hives in treated and untreated sites did not show significantly different quantities of honey over the course of a season.
- For additional protection, urban bee keepers inside the spray zone can cover their hives when spraying occurs.
- Although significant exposure to bees would not occur with Naled application at dawn and dusk, beekeepers can reduce potential exposure to bee colonies even more by covering colonies and preventing bees from exiting during designated treatment periods or, if possible, relocating colonies to an untreated site.
- The spraying of mosquito larvicides will not impact bees.
Will aerial spraying kill birds or other animals?
- No, when aerial spraying is done correctly, it does not harm birds or other animals.
- The insecticides used for aerial spraying do not pose risks to wildlife or the environment.
- Aerial spraying does not cause long-term harm to the environment or local ecosystem, even if spraying happens more than once.
- EPA-registered insecticides used for aerial spraying break down rapidly in the environment, and it displays low toxicity to birds and mammals.
- Aerial spraying will not harm coquis or fish or animals that live in the water. People do not need to cover fish ponds when spraying takes place. If a larvicide is sprayed, it is better if ponds are not covered.
Will Bti affect animals or wildlife?
- No, Bti does not pose a risk to other mammals, birds, or aquatic life, including coqui frogs in Puerto Rico. The toxins it produces only begin working once swallowed by certain insects (larvae of mosquitoes, blackflies, and fungus gnats).
Aerial Spraying and the Environment
Will aerial spraying pollute water?
- No, when aerial spraying is done correctly, it does not pollute water.
- Research shows that, when applied according to label instructions, EPA-registered insecticides sprayed in low levels (about two tablespoons per acre [4,046 square meters]) does not cause long-term harm to the environment or local ecosystem, even if spraying happens more than once.
Will chemicals from aerial spraying contaminate soil?
- No, when chemicals used in aerial spraying are used correctly, they will not contaminate soil.
- Aerial spraying does not cause harm to the environment or local ecosystem, even if spraying happens more than once.
- When applied according to label instructions, EPA-registered insecticides do not pose a risk to human health or the environment.
More information can be found on the US Environmental Protection Agency’s website.
Will Bti affect water sources?
- No. Because Bti has no toxic effect on people, it poses no risk of contamination to water supplies.
Resources
Language:
English
Recommend on FacebookTweet
- Mosquito Life Cycle
- Estimated Range of Aedes aegypti and Aedes albopictus in the United States, 2016
- Controlling Aedes aegypti and Aedes albopictus
Mosquito Control: What you need to know about using larvicides
Mosquito Control: What you need to know about truck-mounted spraying
Mosquito Control: What you need to know about aerial spraying
Mosquito Control: What you need to know about filling tree holes
Mosquito Control: What you need to know about indoor spraying
Mosquito Control: What you need to know about outdoor spraying
Mosquito Control: What you need to know about using adulticides
Mosquito Control: What state and local mosquito control programs do
Did You Know: Important Information about Aerial Spraying for Mosquito Control
Larvicide Dunk Use Wallet Cards
Health Effects & Risks
Language:
English
Recommend on FacebookTweet
What we know
- Zika infection during pregnancy can cause serious birth defects and is associated with other pregnancy problems.
- Several countries that have experienced Zika outbreaks recently have reported increases in people who have Guillain-Barré syndrome (GBS).
- Current CDC research suggests that GBS is strongly associated with Zika; however, only a small proportion of people with recent Zika virus infection get GBS.
MICROCEPHALY & OTHER BIRTH DEFECTS
Zika infection during pregnancy can cause a birth defect called microcephaly, as well as other severe fetal brain defects.
GUILLAIN-BARRÉ SYNDROME
CDC is investigating the link between Zika virus infection and GBS, an uncommon sickness of the nervous system.
Microcephaly & Other Birth Defects
Language:
English
Recommend on FacebookTweet
Zika and microcephaly
Microcephaly is a birth defect where a baby’s head is smaller than expected when compared to babies of the same sex and age. Babies with microcephaly often have smaller brains that might not have developed properly.
Zika virus infection during pregnancy is a cause of microcephaly and other severe fetal brain defects and has been linked to problems in infants, including eye defects, hearing loss, and impaired growth. Scientists are studying the full range of other potential health problems that Zika virus infection during pregnancy may cause.
Other possible causes of microcephaly
Microcephaly can happen for many reasons. Some babies have microcephaly because of
- Changes in their genes
- Certain infections during pregnancy
- A woman being close to or touching toxins during pregnancy
Zika and Other Pregnancy Problems
In addition to microcephaly, other problems have been detected among fetuses and infants infected with Zika virus before birth, such as eye defects, hearing loss, and impaired growth. Although Zika virus is a cause of microcephaly and other severe fetal brain defects and has been linked with these other problems in infants, there is more to learn. Researchers are collecting data to better understand the extent Zika virus impact on mothers and their children.
Future Pregnancies
Based on the available evidence, we think that Zika virus infection in a woman who is not pregnant would not pose a risk for birth defects in future pregnancies after the virus has cleared from her blood. From what we know about similar infections, once a person has been infected with Zika virus, he or she is likely to be protected from a future Zika infection.
Pregnancy
Language:
English
Recommend on FacebookTweet
What we know
What we do not know
- If there’s a safe time during your pregnancy to travel to an area with Zika.
- How likely it is that Zika infection will affect your pregnancy.
- If your baby will have birth defects if you are infected while pregnant.
Zika & Pregnancy in Puerto Rico
Right now, Zika is spreading rapidly in Puerto Rico and pregnant women are at risk for becoming infected with Zika. If current trends continue, at least 1 in 4 people, including women who become pregnant, may become infected with Zika. Since Zika causes microcephaly and other birth defects, it is more important than ever to consider if now is the right time for you to get pregnant. If you decide that now isn’t the right time for you to have a baby, there are contraceptive methods that are safe and effective. If you decide to get pregnant, there are important steps you should take to try to protect yourself from getting Zika.
PREGNANT WOMEN
Learn how to protect yourself and your pregnancy from Zika.
TRYING TO BECOME PREGNANT?
Talk to your doctor or other healthcare provider to plan for a healthy and safe pregnancy.
PREVENTING PREGNANCY
If you decide that now is not the right time to have a baby, talk to your doctor or other healthcare provider.
MICROCEPHALY & OTHER BIRTH DEFECTS
Zika infection during pregnancy can cause a birth defect called microcephaly, as well as other severe fetal brain defects.
PREGNANCY OUTCOMES
Outcomes of pregnancies with laboratory evidence of possible Zika virus infection in the United States.
If you have questions about a possible infection or diagnosis
If families would like to speak to someone about a possible Zika virus infection or diagnosis during pregnancy and risk to the baby, please contact MotherToBaby. MotherToBaby experts are available to answer questions in English or Spanish by phone or chat. The free and confidential service is available Monday-Friday 8am-5pm (local time). To reach MotherToBaby:
- Call 1-866-626-6847
- Chat live or send an email through the MotherToBaby website
Information for Specific Groups
Language:
English
Recommend on FacebookTweet
TRAVELERS
MEDIA
STATE & LOCAL HEALTH DEPARTMENTS
INFORMATION FOR PARENTS
WOMEN TRYING TO BECOME PREGNANT
LAW & POLICYMAKERS
WORKERS
BLOOD AND TISSUE COLLECTION CENTERS
SCHOOLS
Zika Partner Call Information
For more information on Zika announcements, online resources, facts, and guidance, please subscribe to our Emergency Partners newsletterhere
State and Local Health Departments
Language:
English
Recommend on FacebookTweet
Prepare for Zika
Have a Communication Plan
Monitor the Situation
Laboratory Information
More
Clinical Information
More
Communication Resources
CDC offers many free resources like fact sheets and door hangers to help communicate with the public about Zika.
Mosquito Control
Mosquito Bite Prevention
More
Key Health Department Actions
State and local public health agencies can:
- Test for Zika virus or work with CDC’s Arbovirus Diagnostic Laboratory to test for Zika virus when indicated.
- Report laboratory-confirmed cases to CDC through ArboNET, the national surveillance system for arboviral disease.
- Participate in the US Zika Pregnancy Registry.
- Activate or enhance mosquito surveillance and control activities.
Get the Zika Action Sheet
Women Trying to Become Pregnant
Language:
English
Recommend on FacebookTweet
How to protect yourself
CDC recommends special precautions for women and their partners thinking about pregnancy.
What to do if you live in or travel to an area with Zika
If you aren’t pregnant, but you’re thinking about having a baby, here’s what you can do
Talk with your doctor or other healthcare provider
Women and their partners who are thinking about pregnancy should talk with their doctor or healthcare provider about
- Their plans for having children
- The potential risk of getting Zika during pregnancy
- Their partner’s potential exposures to Zika
The table below shows the suggested timeframes for waiting to get pregnant after possible exposure to Zika:
Suggested timeframe to wait before trying to get pregnant
|
| Possible exposure via recent travel or sex without a condom with a man infected with Zika |
|
Women |
Men |
| Zika symptoms |
Wait at least 8 weeks after symptoms start |
Wait at least 6 months after symptoms start |
| No Zika symptoms |
Wait at least 8 weeks after exposure |
Wait at least 8 weeks after exposure.
Talk with your healthcare provider |
| People living in areas with Zika |
|
Women |
Men |
| Zika symptoms |
Wait at least 8 weeks after symptoms start |
Wait at least 6 months after symptoms start |
| No Zika symptoms |
Talk with doctor or healthcare provider |
Talk with doctor or healthcare provider |
Decisions about pregnancy planning are personal and complex, and the circumstances for women and their partners will vary. Women and their partners should discuss pregnancy planning with a trusted doctor or healthcare provider. As part of counseling with healthcare providers, some women and their partners living in areas with active Zika virus transmission might decide to delay pregnancy.
PREVENTING PREGNANCY
If you decide that now is not the right time to have a baby, talk to your doctor or other healthcare provider.
Related Resources
For Women in Areas with Zika: Plan Your Pregnancy
Factsheets & posters
Learn more about Zika with our fact sheets and posters.
More
Pregnant Women
Language:
English
Recommend on FacebookTweet
How to protect yourself
Until we know more, CDC recommends special precautions for pregnant women.
Do not travel to an area with Zika
What to do if you live in or travel to an area with Zika
If you live in an area with Zika, or if you or your sexual partner travel to an area with Zika, follow the steps below to protect your pregnancy.
| If you… |
When to talk with a doctor |
When to be tested |
| Traveled to an area with Zika |
Talk to a doctor or other healthcare provider about your travel even if you don’t feel sick. |
If you have symptoms of Zika within 2 weeks of traveling, you should betested for Zika. |
| If you do not develop symptoms of Zika within 2 weeks of traveling, you should be tested for Zika. |
| Live in an area with Zika |
Talk to a doctor or other healthcare provider throughout your pregnancy. |
You may be at risk of getting Zika throughout your pregnancy. For this reason, doctors or other healthcare providers can offer testing
- At the first prenatal visit and
- A second test in the second trimester.
If you have symptoms of Zika at any time during your pregnancy, you should be tested for Zika. |
Items to discuss with your doctor or other healthcare provider
See your doctor or other healthcare provider if you have the symptoms described above and have visited or live in an area with Zika.
Doctor’s Visit Checklist: For Pregnant Women Who Traveled to an Area with Zika
Doctor’s Visit Checklist: For Pregnant Women Living in an Area with Zika
Zika virus testing for pregnant women living in an area with Zika
Zika Virus Testing for Any Pregnant Woman Not Living in an Area With Zika
If you test positive for Zika
A positive test result might cause concerns, but it doesn’t mean your baby will have birth defects.
For Pregnant Women: A Positive Zika Virus Test: What does it mean for me?
If you test positive for Zika and live in the U.S.
To understand more about Zika virus infection, CDC established the US Zika Pregnancy Registry and is collaborating with state, tribal, local, and territorial health departments to collect information about pregnancy and infant outcomes following laboratory evidence of Zika virus.
Fact Sheet for Pregnant Women
Related Resources
Pregnant? Read this before you travel
Pregnant and living in an area with Zika?
For pregnant women in areas with Zika: Protect your pregnancy
Pregnant? Protect yourself from mosquito bites
Zika and Sex: Information for pregnant women living in areas with Zika
Zika and Sex: Information for men who have pregnant partners and live in or recently traveled to areas with Zika
Factsheets & posters
Learn more about Zika with our fact sheets and posters.
More
Preventing Unintended Pregnancy during the Zika Virus Outbreak
Language:
English
Recommend on FacebookTweet
CDC is providing this information because Zika virus infection during pregnancy can cause a birth defect of the brain called microcephaly and other severe fetal brain defects.
How to Prevent Unintended Pregnancy
If you decide that now is not the right time to have a baby, talk to your doctor or other healthcare provider. The best way to prevent unintended pregnancy if you are sexually active is to use an effective form of birth control the right way, every time you have sex. It is important to find a type of birth control that is safe, effective, and works for you.
Types of Birth Control
There are many different types of birth control; some have hormones and some don’t. Also, some methods are permanent while others are reversible. The most effective reversible birth control is long-acting reversible contraception (LARC), which includes intrauterine devices (IUDs) and implants. LARC are highly effective for years and once correctly in place, require no action on your part, but can be removed at any time if you decide you want to become pregnant.
For other types of birth control, the effectiveness depends on using them correctly and consistently—so these methods have lower effectiveness with typical use. These methods include
- Hormonal methods (contraceptive shot, pills, patch, and ring)
- Barrier methods (condoms, diaphragms, spermicides)
- Methods based on understanding your monthly fertility pattern
You can use this chart (Spanish version) to look at the full range of birth control options and understand which one best fits your lifestyle and needs.
PUBLIC HEALTH LAW PROGRAM
Zika Resources
Recommend on FacebookTweet
Response to the Zika virus disease (Zika) requires an understanding of complex public health issues, including the role of law in controlling the spread of infectious diseases. This page provides resources and information developed by the Public Health Law Program to address potential questions from responders and the public about Zika-related legal issues.
- Presentation: Using Policy to Increase Public Understanding and Enhance State and Community Readiness
Zika Action Plan Summit session on using policy to increase public understanding and enhancing state and community readiness. Download[PDF – 1.90MB] the presentation slides.
- Webinar: The Zika Virus: Current Public Health Considerations and What You Need to Know
This webinar provides analysis of the ever-changing state of the Zika virus, including the most prevalent locations and common causes leading the virus to spread, and the latest best practice approach to diagnosing, preventing, and controlling the virus. The webinar also includes legal frameworks for responding to the Zika virus, such as proper disease reporting, vector control, and emergency declarations, and up-to-date domestic and international policy response.
- Webinar: Zika Preparedness and Response: A Public Health and Legal Perspective
This webinar, co-sponsored by the Partnership for Public Health Law, the American Public Health Association, the Association of State and Territorial Health Officials, the National Association of County and City Health Officials, and the National Association of Local Boards of Health, provides an overview of the public health problem posed by Zika, discusses the domestic legal framework for addressing the virus, and highlights ways to coordinate health care and public health legal preparedness. (03/18/2016)
- Executive Orders and Emergency Declarations for the West Nile Virus: Applying Lessons from Past Outbreaks to Zika[PDF – 416KB]
A brief analysis of select uses of local, state, and federal executive powers to combat the West Nile virus. Examining the use of executive powers to address the West Nile virus may inform actions taken to address the threats posed by other mosquito-borne diseases, such as the Zika virus.
- Zika Virus Microsite
CDC has created the Zika Virus Microsite, an easily embeddable collection of Zika virus information about developments in the current outbreak, including prevention, symptoms, treatment, and materials for travelers and pregnant women.
MEDIA
CDC Newsroom
Zika Virus
Language:
English
Recommend on FacebookTweet
Zika virus spreads to people primarily through the bite of an infected Aedes species mosquito (Ae. aegypti and Ae. albopictus), but can also be spread during sex by a person infected with Zika to his or her sex partners. Many people infected with Zika won’t have symptoms, but for those who do, the illness is usually mild with symptoms lasting from several days to a week. The most common symptoms of Zika are fever, rash, joint pain, and conjunctivitis (red eyes). Severe disease requiring hospitalization is uncommon. However, Zika infection during pregnancy can cause a serious birth defect of the brain called microcephaly and other severe fetal brain defects. Until more is known, CDC recommends that pregnant women avoid traveling to areas with Zika.
Outbreaks of Zika are occurring in many countries and territories, and because the mosquitoes that spread Zika virus are found throughout the world, it is likely that outbreaks will spread to new countries. On Feb. 1, 2016 the World Health Organization (WHO) declared a Public Health Emergency of International Concern because of clusters of microcephaly and other neurological disorders in some areas affected by Zika. lLab tests have confirmed Zika virus in travelers returning to the United States and in some non-travelers who got Zika through sex with a traveler. Local transmission of Zika virus has been reported in the United States(http://www.cdc.gov/zika/geo/united-states.html). Additionally, local transmission of Zika has been reported in US territories, including the Commonwealth of Puerto Rico, the US Virgin Islands, and American Samoa.
What CDC is doing
CDC’s Emergency Operations Center is activated at Level 1, its highest level, to respond to the Zika outbreak. CDC is working with public health partners and with state, local, and territorial health departments to alert healthcare providers and the public about Zika; post travel notices and other travel-related guidance; provide state health laboratories with diagnostic tests; monitor and report cases of Zika; publish guidelines to inform testing and treatment of people with suspected or confirmed Zika; study what might be responsible for the reported rise in microcephaly; and working with partners around the world to develop a better understanding of Zika virus.
Related Links
Most Relevant
Science Behind the Issue
Multimedia
http://www.cdc.gov/niosh/topics/outdoor/mosquito-borne/zika.html
Zika Virus
Recommend on FacebookTweet
Key Worker Resources
OSHA/NIOSH Interim Guidance for Protecting Workers from Occupational Exposure to Zika Virus
NIOSH Zika: Protecting Outdoor Workers
NIOSH Zika: Protecting US Businesses and Business Travelers
NIOSH Zika: Protecting Healthcare and Laboratory Workers
Reminder about Preventing Sharps Injuries and the Zika Virus
Zika virus disease (Zika) is caused by the Zika virus and is spread to people primarily from the bite of an infected Aedes species mosquito. These mosquitoes bite most actively in the daytime but also bite at night. There is currently no vaccine to prevent Zika infection.
NIOSH and OSHA developed guidance for protecting workers from occupational exposure to Zika virus. NIOSH has also developed fact sheets for outdoor workers, U.S. businesses and business travelers, healthcare and laboratory workers, and a fact sheet and poster for cruise ship workers. For updated Zika information visit CDC Zika.
What are the symptoms?
Where are workers at risk?
Workers at risk include those who work in or travel to areas with Zika . Local transmission of Zika virus has been reported in two areas of Miami, Florida, three U.S. territories: the Commonwealth of Puerto Rico, the U.S. Virgin Islands, and American Samoa, and multiple countries . For the most current information about where Zika is found, visit the CDC Areas with Zika and Zika Travel Information.
Those who work or travel in an area with Zika should take steps to prevent Zika
Are pregnant women at special risk?
- Pregnant women should NOT travel to an area with active Zika virus transmission.
- Pregnant women, women who may become pregnant, and people with sexual partners who are or may become pregnant should talk to their healthcare providers about the risk of Zika.
- For additional updated information visit CDC Zika pregnancy.
USAID Zika Grand Challenge for Development
The U.S. Agency for International Development (USAID) launched “Combating Zika and Future Threats: A Grand Challenge for Development” to encourage ideas and innovations to help reduce the spread and impact of Zika virus and other infectious disease outbreaks. Initial results of the Grand Challenge are available.
Resources
- CDC Zika Virus
About Zika virus, areas with Zika, symptoms, diagnosis, treatment, prevention, transmission, surveillance, and more.
- OSHA/NIOSH Interim Guidance for Protecting Workers from Occupational Exposure to Zika Virus
Provides employers and workers with information about preventing workplace exposure.
Español
- NIOSH Zika: Protecting Outdoor Workers
Fact sheet for outdoor workers.
- NIOSH Zika: Protecting US Businesses and Business Travelers
Fact sheet for businesses and business travelers.
- NIOSH Zika: Protecting Healthcare and Laboratory Workers
Fact sheet for healthcare and laboratory workers.
- NIOSH Fact Sheet for Cruise Line Employees: Prevent Mosquito-borne Diseases
Fact sheet for cruise line workers.
- NIOSH Poster for Cruise Line Employees: Prevent Mosquito Bites
Poster for cruise line workers.
- NIOSH Science Blog:
Zika and Olympic Work
- OSHA Zika Virus
Provides workplace information for employers and workers.
- OSHA QuickCard: Zika Virus Protection for Outdoor Workers
Information for outdoor workers and employers in card format.
Español
- CDC Statement on Disinsection
CDC does not recommend the routine use of insecticides (disinsection) inside commercial passenger airplanes to prevent the spread of Zika virus.
- CDC Zika Virus – For Pregnant Women
Zika virus can be spread from a pregnant woman to her fetus and has been linked to a serious birth defect of the brain called microcephaly.
- Biosafety Guidance for Transportation of Specimens and for Work with Zika Virus in the Laboratory
Provides laboratory safety recommendations for transport and handling of diagnostic specimens and laboratory work.
- NIOSH Needlestick and Sharps Injuries Information: Bloodborne Infectious Diseases
Provides prevention, management, and emergency information for needlestick and sharps injuries.
- CDC Zika Travel Information
Travel notices, information for travelers and clinicians.
- CDC Zika Virus – Fact Sheets and Posters
Fact sheets and posters available as PDFs.
- NIOSH Fast Facts: Protecting Yourself from Ticks and Mosquitoes
Print or order this free card for easy access to important safety information.
- CDC Zika Virus – For Healthcare Providers
Provides information about clinical evaluation and testing.
- MMWR Zika Reports
Comprehensive resource for CDC Zika reports.
- World Health Organization Zika Virus
Provides global updates and recommendations.
Related Topics
State and Local Health Departments
Language:
English
Recommend on FacebookTweet
Prepare for Zika
Have a Communication Plan
Monitor the Situation
Laboratory Information
More
Clinical Information
More
Communication Resources
CDC offers many free resources like fact sheets and door hangers to help communicate with the public about Zika.
Mosquito Control
Mosquito Bite Prevention
More
Key Health Department Actions
State and local public health agencies can:
- Test for Zika virus or work with CDC’s Arbovirus Diagnostic Laboratory to test for Zika virus when indicated.
- Report laboratory-confirmed cases to CDC through ArboNET, the national surveillance system for arboviral disease.
- Participate in the US Zika Pregnancy Registry.
- Activate or enhance mosquito surveillance and control activities.
Get the Zika Action Sheet
Blood & Tissue Collection Centers
Language:
English
Recommend on FacebookTweet
ZIKA & BLOOD TRANSFUSION
AREAS AT RISK
Guidance
Additional Resources
CDC is working with our partners to learn more about Zika and blood/tissue safety
Just for Kids
Zika Activity Book: For kids in areas with Zika
Zika Activity Book: For kids in the US
Parents
Language:
English
Recommend on FacebookTweet
WHAT PARENTS SHOULD KNOW
MICROCEPHALY
ZIKA AND PREGNANCY
TRAVEL INFORMATION
Planning a pregnancy?
See CDC’s recommendations for couples thinking about pregnancy
Additional Resources
Areas with Zika
Ideas for Talking to your Child About Zika
Protecting Children in Puerto Rico from Zika
What Parents Should Know about Zika
Language:
English
Recommend on FacebookTweet
What we know about Zika
- Infants and children can be infected with Zika.
- The primary way that infants and children get Zika is through bites of two types of mosquitoes. Information on safely preventing mosquito bites can be found below or at CDC’s Avoid Mosquito Bites page.
- To date, no cases of Zika have been reported from breastfeeding. Because of the benefits of breastfeeding, mothers are encouraged to breastfeed, even in areas where Zika virus is found.
- Common symptoms of Zika are fever, rash, joint pain, and red eyes. Symptoms usually go away within a few days to one week. Many people infected with Zika don’t have symptoms.
- There is no vaccine or medicine for Zika. For more information about treatment and prevention.
- Birth defects, including microcephaly, and other problems have been reported in babies born to women infected with Zika during pregnancy.
- Zika virus can be passed from a woman to her fetus during pregnancy or around the time of birth. We are studying how Zika virus affects pregnancies.
- Since May 2015, Brazil has had a large outbreak of Zika. During this outbreak, Brazilian officials reported an increase in the number of babies born with microcephaly in areas with Zika. Recently, CDC concluded that Zika virus infection during pregnancy is a cause of microcephaly and other severe fetal brain defects.
- Pregnancy loss and other pregnancy problems have been reported in women infected with Zika during pregnancy. Zika has been linked with other birth defects, including eye defects, hearing loss, and impaired growth.
- Not all babies whose mothers had Zika during pregnancy are born with health problems. Researchers are working to better understand how often having Zika during pregnancy causes problems.
- Infection with Zika virus at later times, including around the time of birth or in early childhood, has not been linked to microcephaly.
- Microcephaly happens for many reasons, and many times the cause is unknown.
- Genetic conditions, certain infections, and toxins can cause microcephaly. If your child has microcephaly, his or her doctor or other healthcare provider will look for the underlying reason. However, for about half of children with microcephaly, the underlying cause is never discovered.
- If you have a child with microcephaly, it is unlikely that it had to do with Zika if you did not travel to an area with Zika during pregnancy.
- Although head size reflects brain size, head size does not always predict short- or long-term health effects. While some children with microcephaly can have seizures, vision or hearing problems, and developmental disabilities, others do not have health problems.
What we don’t know about Zika
- We do not know how often Zika is passed from a woman to her fetus during pregnancy or around the time of birth.
- We do not know whether the timing of the woman’s Zika virus infection during pregnancy, or the severity of a woman’s symptoms, affect her pregnancy.
- We do not know the long-term health outcomes for infants and children with Zika virus infection.
What CDC is doing to learn more
- Developing laboratory tests to diagnose Zika as quickly as possible.
- Conducting research on the link between Zika and microcephaly.
- Identifying new areas with Zika and establishing a US Zika Pregnancy Registry to improve our understanding of the how Zika affects mothers and their children.
- Testing different mosquito species to find out whether they carry Zika.
- Providing advice to US travelers returning from areas with current outbreaks; and, supporting US states and territories already affected by Zika.
- Preparing states and Americans with prevention actions in advance of mosquito season.
What parents can do
- Prevent mosquito bites.
To protect your child from mosquito bites
- Dress your child in clothing that covers arms and legs.
- Cover crib, stroller, and baby carrier with mosquito netting.
- Do not use insect repellent on babies under 2 months of age.
- Do not use products containing oil of lemon eucalyptus or para-menthane-diol on children younger than 3 years old.
- In children older than 2 months, do not apply insect repellent onto a child’s hands, eyes, mouth, or to irritated or broken skin.
- Never spray insect repellent directly on a child’s face. Instead, spray it on your hands and then apply sparingly, taking care to avoid the eyes and mouth.
- Control mosquitoes inside and outside your home.
- If your child has symptoms, take him or her to see a doctor or other healthcare provider.
For children with Zika symptoms of fever, rash, joint pain, or red eyes who have traveled to or resided in an affected area, contact your child’s health care provider and describe where you have traveled.
- Fever (≥100.4° F) in a baby less than 2 months old always requires evaluation by a medical professional. If your baby is less than 2 months old and has a fever, call your health care provider or get medical care.
Additional Resources
Facts about Microcephaly
Language:
English
Recommend on FacebookTweet
Click here to view a larger image
Microcephaly is a birth defect where a baby’s head is smaller than expected when compared to babies of the same sex and age. Babies with microcephaly often have smaller brains that might not have developed properly.
What is microcephaly?
Microcephaly is a condition where a baby’s head is much smaller than expected. During pregnancy, a baby’s head grows because the baby’s brain grows. Microcephaly can occur because a baby’s brain has not developed properly during pregnancy or has stopped growing after birth, which results in a smaller head size. Microcephaly can be an isolated condition, meaning that it can occur with no other major birth defects, or it can occur in combination with other major birth defects.
What is severe microcephaly?
Severe microcephaly is a more serious, extreme form of this condition where a baby’s head is much smaller than expected. Severe microcephaly can result because a baby’s brain has not developed properly during pregnancy, or the brain started to develop correctly and then was damaged at some point during pregnancy.
Other Problems
Babies with microcephaly can have a range of other problems, depending on how severe their microcephaly is. Microcephaly has been linked with the following problems:
- Seizures
- Developmental delay, such as problems with speech or other developmental milestones (like sitting, standing, and walking)
- Intellectual disability (decreased ability to learn and function in daily life)
- Problems with movement and balance
- Feeding problems, such as difficulty swallowing
- Hearing loss
- Vision problems
These problems can range from mild to severe and are often lifelong. Because the baby’s brain is small and underdeveloped, babies with severe microcephaly can have more of these problems, or have more difficulty with them, than babies with milder microcephaly. Severe microcephaly also can be life-threatening. Because it is difficult to predict at birth what problems a baby will have from microcephaly, babies with microcephaly often need close follow-up through regular check-ups with a healthcare provider to monitor their growth and development.
Occurrence
Microcephaly is not a common condition. State birth defects tracking systems have estimated that microcephaly ranges from 2 babies per 10,000 live births to about 12 babies per 10,000 live births in the Unites States.1
Causes and Risk Factors
The causes of microcephaly in most babies are unknown. Some babies have microcephaly because of changes in their genes. Other causes of microcephaly, including severe microcephaly, can include the following exposures during pregnancy:
- Certain infections during pregnancy, such as rubella, toxoplasmosis, or cytomegalovirus
- Severe malnutrition, meaning a lack of nutrients or not getting enough food
- Exposure to harmful substances, such as alcohol, certain drugs, or toxic chemicals
- Interruption of the blood supply to the baby’s brain during development
Some babies with microcephaly have been reported among mothers who were infected with Zika virus while pregnant. CDC scientists announced that enough evidence has accumulated to conclude that Zika virus infection during pregnancy is a cause of microcephaly and other severe fetal brain defects.
CDC continues to study birth defects, such as microcephaly, and how to prevent them. If you are pregnant or thinking about becoming pregnant, talk with your doctor about ways to increase your chances of having a healthy baby.
Zika Virus and Pregnancy
For information about the effects of Zika virus infection during pregnancy, visit CDC’s Zika and Pregnancy web page.
Diagnosis
Microcephaly can be diagnosed during pregnancy or after the baby is born.
During Pregnancy
During pregnancy, microcephaly can sometimes be diagnosed with an ultrasound test (which creates pictures of the body). To see microcephaly during pregnancy, the ultrasound test should be done late in the 2nd trimester or early in the third trimester. For more information about screening and confirmatory tests during pregnancy, visit CDC’s birth defects diagnosis web page.
After the Baby is Born
To diagnose microcephaly after birth, a healthcare provider will measure the distance around a newborn baby’s head, also called the head circumference, during a physical exam. The provider then compares this measurement to population standards by sex and age. Microcephaly is defined as a head circumference measurement that is smaller than a certain value for babies of the same age and sex. This measurement value for microcephaly is usually less than 2 standard deviations (SDs) below the average. The measurement value also may be designated as less than the 3rd percentile. This means the baby’s head is extremely small compared to babies of the same age and sex.
Head circumference growth charts for newborns, infants, and children up to age 20 years in the United States can be found on CDC’s growth charts website. Head circumference growth charts based on gestational age at birth (in other words, how far along the pregnancy was at the time of delivery) are also available from INTERGROWTH 21st. CDC recommends that health care providers use the WHO growth charts to monitor growth for infants and children ages 0 to 2 years of age in the United States.
Often, healthcare providers should take the head circumference measurement when the newborn baby is at least 24 hours old. This helps make sure that compression due to delivery through the birth canal has resolved. If the healthcare provider suspects the baby has microcephaly, he or she can request one or more tests to help confirm the diagnosis. For example, special tests like a CT scan or an MRI can provide critical information on the structure of the baby’s brain that can help determine if the newborn baby had an infection during pregnancy. They also can help the healthcare provider look for other problems that might be present.
Webinar on Surveillance
Download slides | Download transcript
Treatments
Microcephaly is a lifelong condition. There is no known cure or standard treatment for microcephaly. Because microcephaly can range from mild to severe, treatment options can range as well. Babies with mild microcephaly often don’t experience any other problems besides small head size. These babies will need routine check-ups to monitor their growth and development.
For more severe microcephaly, babies will need care and treatment focused on managing their other health problems (mentioned above). Developmental services early in life will often help babies with microcephaly to improve and maximize their physical and intellectual abilities. These services, known as early intervention, can include speech, occupational, and physical therapies. Sometimes medications also are needed to treat seizures or other symptoms.
Other Resources
The views of these organizations are their own and do not reflect the official position of CDC.
Mother To Baby (on behalf of the Organization of Teratology Information Specialists)
This website provides comprehensive information to mothers, healthcare professionals, and the general public about exposures during pregnancy.
References
- National Birth Defects Prevention Network. Major birth defects data from population-based birth defects surveillance programs in the United States, 2006-2010. Birth Defects Research (Part A): Clinical and Molecular Teratology. 2013;97:S1-S172.
Health Effects & Risks
Language:
English
Recommend on FacebookTweet
What we know
- Zika infection during pregnancy can cause serious birth defects and is associated with other pregnancy problems.
- Several countries that have experienced Zika outbreaks recently have reported increases in people who have Guillain-Barré syndrome (GBS).
- Current CDC research suggests that GBS is strongly associated with Zika; however, only a small proportion of people with recent Zika virus infection get GBS.
MICROCEPHALY & OTHER BIRTH DEFECTS
Zika infection during pregnancy can cause a birth defect called microcephaly, as well as other severe fetal brain defects.
Microcephaly & Other Birth Defects
Language:
English
Recommend on FacebookTweet
Zika and microcephaly
Microcephaly is a birth defect where a baby’s head is smaller than expected when compared to babies of the same sex and age. Babies with microcephaly often have smaller brains that might not have developed properly.
Zika virus infection during pregnancy is a cause of microcephaly and other severe fetal brain defects and has been linked to problems in infants, including eye defects, hearing loss, and impaired growth. Scientists are studying the full range of other potential health problems that Zika virus infection during pregnancy may cause.
Other possible causes of microcephaly
Microcephaly can happen for many reasons. Some babies have microcephaly because of
- Changes in their genes
- Certain infections during pregnancy
- A woman being close to or touching toxins during pregnancy
Zika and Other Pregnancy Problems
In addition to microcephaly, other problems have been detected among fetuses and infants infected with Zika virus before birth, such as eye defects, hearing loss, and impaired growth. Although Zika virus is a cause of microcephaly and other severe fetal brain defects and has been linked with these other problems in infants, there is more to learn. Researchers are collecting data to better understand the extent Zika virus impact on mothers and their children.
Future Pregnancies
Based on the available evidence, we think that Zika virus infection in a woman who is not pregnant would not pose a risk for birth defects in future pregnancies after the virus has cleared from her blood. From what we know about similar infections, once a person has been infected with Zika virus, he or she is likely to be protected from a future Zika infection.
Zika and Guillain-Barré Syndrome
Recommend on FacebookTweet
Guillain-Barré syndrome (GBS) is an uncommon sickness of the nervous system in which a person’s own immune system damages the nerve cells, causing muscle weakness, and sometimes, paralysis.
- Several countries that have experienced Zika outbreaks recently have reported increases in people who have Guillain-Barré syndrome (GBS).
- Current CDC research suggests that GBS is strongly associated with Zika; however, only a small proportion of people with recent Zika virus infection get GBS.
CDC is continuing to investigate the link between GBS and Zika to learn more.
Symptoms of GBS
GBS symptoms include weakness of the arms and legs and, in severe cases, can affect the muscles that control breathing.
These symptoms can last a few weeks or several months. Most people fully recover from GBS, though some people have permanent damage. Very few people die from GBS.
Causes of GBS
Researchers do not fully understand what causes GBS. Most people with GBS report an infection before they have GBS symptoms. Rarely, vaccination has also been associated with the onset of GBS (for example, the 1976 Swine influenza vaccine).
GBS is rare
An estimated 3,000 to 6,000 people, or 1-2 cases for every 100,000 people, develop GBS each year in the US. Most cases of GBS tend to occur for no known reason, and true “clusters” of cases of GBS are very unusual.
What to do if you are concerned
If you want to know more about the number of GBS cases in a certain area, contact the state or local health department in the state where the cases happen. CDC collaborates with state and local health departments to investigate reports of possibly unusually large numbers or “clusters” of GBS cases.
Additional Resources
Vaccine Safety Concerns- Guillain-Barré Syndrome
Guillain-Barré syndrome and Flu Vaccine: Questions and Answers
Zika Travel Information
Recommend on FacebookTweet
Language:
Select
Note: The information on this page is for travelers to international destinations and US territories. For information on Zika in US states, visit Areas with Zika. For the most current information about Zika virus, please visit CDC’s Zika website.
Traveling soon? Get Zika info on-the-go.
Sign up to receive Zika updates for your destination with CDC’s new text messaging service. Text PLAN to 855-255-5606 to subscribe.
Zika Travel Notices
- Zika Virus in Cape Verde
- Zika Virus in Mexico
- Asia
Currently includes: Singapore
- The Caribbean
Currently includes: Anguilla; Antigua and Barbuda; Aruba; The Bahamas; Barbados; Bonaire; British Virgin Islands; Cayman Islands;Cuba; Curaçao; Dominica; Dominican Republic; Grenada; Guadeloupe;Haiti; Jamaica; Martinique; the Commonwealth of Puerto Rico, a US territory; Saba; Saint Barthelemy; Saint Lucia; Saint Martin; Saint Vincent and the Grenadines; Sint Eustatius; Sint Maarten; Trinidad and Tobago; Turks and Caicos Islands; US Virgin Islands
- Central America
Currently includes: Belize, Costa Rica, El Salvador, Guatemala,Honduras, Nicaragua, Panama
- The Pacific Islands
Currently includes: American Samoa, Fiji, Marshall Islands, Micronesia,New Caledonia, Papua New Guinea, Samoa, Tonga
- South America
Currently includes: Argentina, Bolivia, Brazil, Colombia, Ecuador, French Guiana, Guyana, Paraguay, Peru, Suriname, Venezuela
- 2016 Summer Olympics (Rio 2016)
Countries with Endemic Zika
Some countries in Africa, the Pacific Islands, and Asia have reported Zika in the past and may continue to occasionally report new cases. The risk to travelers in these endemiccountries is likely much lower than it is in countries with Zika epidemics (see Q&A: Zika Risk in Countries with Endemic Zika). Because Zika infection in a pregnant woman causes severe birth defects, pregnant women should consult with their health care provider and, if they decide to travel, strictly follow steps to prevent mosquito bites. Travel notices have not been issued for these destinations but would be considered if the number of cases rises to the level of an outbreak. Check this page for the most up-to-date information before you make travel plans.
Africa: Angola, Benin, Burkina-Faso, Cameroon, Central African Republic, Côte d’Ivoire, Egypt, Ethiopia, Gabon, Guinea-Bissau, Kenya, Liberia, Mali, Mozambique, Niger, Nigeria, Senegal, Sierra Leone, Somalia, Tanzania, Togo, Uganda, Zambia
Asia: Bangladesh, Cambodia, India, Indonesia, Malaysia, Maldives, Pakistan, Philippines, Thailand, Vietnam
The Pacific Islands: Easter Island, Vanuatu
Special Populations
Countries and territories with travel notices reporting active mosquito transmission of Zika virus. Click to enlarge
For Clinicians
Empaca para prevenir el Zika (video en español)
Infographic: #ZIKA Team USA’s Prevention Playbook.
For Healthcare Providers
Language:
English
Recommend on FacebookTweet
Zika virus disease is a nationally notifiable condition. Healthcare providers should report suspected Zika virus disease cases to their state, local, or territorial health department to facilitate diagnosis and mitigate risk of local transmission. State, local, and territorial health departments should report laboratory-confirmed and probable cases to CDC.
Clinical Guidance
Testing for Zika
Overview & Training
Key Considerations for Healthcare Settings
More Resources
Clinical Evaluation & Disease
Language:
English
Recommend on FacebookTweet
Modes of Transmission
Zika virus is a single-stranded RNA virus of the Flaviviridae family, genus Flavivirus. Zika virus is transmitted to humans primarily through the bite of an infected Aedes species mosquito (Ae. aegypti and Ae. albopictus). The mosquito vectors typically breed in domestic water-holding containers; they are aggressive daytime biters and feed both indoors and outdoors near dwellings. Nonhuman and human primates are likely the main reservoirs of the virus, and anthroponotic (human-to-vector-to-human) transmission occurs during outbreaks.
Perinatal, in utero, and possible sexual and transfusion transmission events have also been reported. Zika virus RNA has been identified in asymptomatic blood donors during an ongoing outbreak.
Clinical Signs & Symptoms
Many people infected with Zika virus are asymptomatic. Characteristic clinical findings are acute onset of fever with maculopapular rash, arthralgia, or conjunctivitis. Other commonly reported symptoms include myalgia and headache. Clinical illness is usually mild with symptoms lasting for several days to a week. Severe disease requiring hospitalization is uncommon and case fatality is low. However, there have been cases of Guillain-Barré syndrome reported in patients following suspected Zika virus infection. Recently, CDC concluded that Zika virus infection during pregnancy is a cause of microcephaly and other severe fetal brain defects. Due to concerns of microcephaly caused by maternal Zika virus infection, fetuses and infants of women infected with Zika virus during pregnancy should be evaluated for possible congenital infection and neurologic abnormalities.
Diagnosis & Reporting
Based on the typical clinical features, the differential diagnosis for Zika virus infection is broad. In addition to dengue, other considerations include leptospirosis, malaria, rickettsia, group A streptococcus, rubella, measles, and parvovirus, enterovirus, adenovirus, and alphavirus infections (e.g., chikungunya, Mayaro, Ross River, Barmah Forest, o’nyong-nyong, and sindbis viruses).
Preliminary diagnosis is based on the patient’s clinical features, places and dates of travel, and activities. Laboratory diagnosis is generally accomplished by testing serum or plasma to detect virus, viral nucleic acid, or virus-specific immunoglobulin M and neutralizing antibodies.
As an arboviral disease, Zika virus is a nationally notifiable condition. Healthcare providers are encouraged to report suspected cases to their state or local health departments to facilitate diagnosis and mitigate the risk of local transmission. State or local health departments are encouraged to report laboratory-confirmed cases to CDC through ArboNET, the national surveillance system for arboviral disease.
Treatment
No specific antiviral treatment is available for Zika virus disease. Treatment is generally supportive and can include rest, fluids, and use of analgesics and antipyretics. Because of similar geographic distribution and symptoms, patients with suspected Zika virus infections also should be evaluated and managed for possible dengue or chikungunya virus infection. Aspirin and other non-steroidal anti-inflammatory drugs (NSAIDs) should be avoided until dengue can be ruled out to reduce the risk of hemorrhage. People infected with Zika, chikungunya, or dengue virus should be protected from further mosquito exposure during the first few days of illness to prevent other mosquitoes from becoming infected and reduce the risk of local transmission.
Clinical Guidance
Language:
English
Recommend on FacebookTweet
In this Section
Updated Clinical Guidance
Key Considerations for Healthcare Settings
More Resources
US Zika Pregnancy Registry
Language:
English
Recommend on FacebookTweet
If you have questions about a possible infection or diagnosis
If families would like to speak to someone about a possible Zika virus infection or diagnosis during pregnancy and risk to the baby, please contact MotherToBaby. MotherToBaby experts are available to answer questions in English or Spanish by phone or chat. The free and confidential service is available Monday – Friday from 8am – 5pm (local time). To reach MotherToBaby:
- Call 1-866-626-6847
- Chat live or send an email through theMotherToBaby website
Zika virus infection during pregnancy can cause microcephaly and other severe fetal brain defects. Infection during pregnancy has also been linked to adverse outcomes including pregnancy loss, and eye defects, hearing loss, and impaired growth in infants. Despite these observations, many questions remain about the risks of Zika virus infection during pregnancy. Information about the timing, absolute risk, and spectrum of outcomes associated with Zika virus infection during pregnancy is needed to direct public health action related to Zika virus and guide testing, evaluation, and management.
To understand more about Zika virus infection, CDC established the US Zika Pregnancy Registry and is collaborating with state, tribal, local, and territorial health departments to collect information about pregnancy and infant outcomes following laboratory evidence of Zika virus infection during pregnancy. The data collected through this registry will be used to update recommendations for clinical care, to plan for services for pregnant women and families affected by Zika virus, and to improve prevention of Zika virus infection during pregnancy.
- If you are a healthcare provider or health department and you have questions about the registry, please email or call 770-488-7100 and ask for the Zika Pregnancy Hotline.
Eligibility for the Registry
People who are eligible for inclusion in the Registry include
- Pregnant women in the United States with laboratory evidence of Zika virus infection (positive or equivocal test results, regardless of whether they have symptoms) and periconceptionally, prenatally or perinatally exposed infants born to these women.
- Infants with laboratory evidence of congenital Zika virus infection (positive or equivocal test results, regardless of whether they have symptoms) and their mothers.
Health Departments: How to Participate
State, tribal, local, and territorial health departments can participate in the US Zika Pregnancy Registry. They can
- Identify pregnant women and infants eligible for Zika virus testing in accordance with state or CDC guidelines.
- Coordinate testing at a state public health laboratory or CDC for those eligible.
- Report information about pregnant women in the United States with laboratory evidence of Zika virus infection (positive or equivocal test results, regardless of whether they have symptoms) and information about periconceptionally, prenatally or perinatally exposed infants born to these women, including infants with congenital Zika virus infection
- Collect enhanced surveillance data about pregnant women and their infants who are eligible for the Registry.
- Work with CDC to determine state-specific methods for collecting and sharing data.
Healthcare Providers: How to Participate
CDC and state, tribal, local, and territorial health departments request that healthcare providers participate in the US Zika Pregnancy Registry.
Obstetric healthcare providers can:
- Report information about pregnant women with laboratory evidence of Zika virus to their state, tribal, local, or territorial health department.
- Collect pertinent clinical information about pregnant women and their infants on the Pregnancy and Zika Virus Disease Surveillance forms.
- Provide the information to state, tribal, local or territorial health departments or directly to CDC registry staff if asked to do so by local health officials.
- Notify state, tribal, local, or territorial health department staff or CDC registry staff of adverse events (e.g., spontaneous abortion, termination of pregnancy).
Pediatric healthcare providers can:
- Identify and report suspected congenital Zika virus exposure to their state, tribal, local, or territorial health department for possible testing.
- Collect pertinent clinical information about infants born to women with laboratory evidence of Zika virus infection or infants with congenital Zika virus infection.
- Provide the information to state, tribal, local or territorial health departments or directly to CDC registry staff if asked to do so by local health officials.
- Notify state, tribal, local, or territorial health department staff or CDC registry staff of adverse events (e.g., perinatal or infant deaths).
Healthcare providers practicing in Puerto Rico should report information to the Puerto Rico Zika Active Pregnancy Surveillance System (ZAPSS) rather than to the US Zika Pregnancy Registry.
Fact Sheets
Fact Sheet for Obstetric Healthcare Providers
Fact Sheet for Pregnant Women
Fact Sheet for Pediatric Healthcare Providers
Fact Sheet for Health Departments
Fact Sheet for Parents
Fact Sheet for Tribal Healthcare Providers
Additional Resources
Zika Active Pregnancy Surveillance System (ZAPSS)/Sistema de Vigilancia Activa de Zika en Embarazos (SVAZE)
Language:
English
Recommend on FacebookTweet
Summary
The Puerto Rico Department of Health and Centers for Disease Control and Prevention have developed a surveillance system called Zika Active Pregnancy Surveillance System (ZAPSS)/Sistema de Vigilancia Activa de Zika en Embarazos (SVAZE). The surveillance system will be used to evaluate the association between Zika virus infection during pregnancy and adverse outcomes during pregnancy, birth, and early childhood up to 3 years old. Pregnant women in Puerto Rico with laboratory evidence of Zika virus infection (positive or inconclusive test results, regardless of whether they have symptoms) and prenatally or perinatally exposed infants born to these women will be actively monitored. This information will be used to inform best practices in care for women infected with Zika virus during pregnancy and their infants.
Where to get more information
For general information, go to CDC’s Zika webpage for pregnant women. For clinical inquiries only, please e-mail ZikaMCH@… or call 770-448-7100 (24/7).
To notify the Puerto Rico Department of Health Birth Defects Surveillance and Prevention System’s staff of any pregnancy outcomes among Zika positive pregnant women, please call: (787) 765-2929 ext. 4571, or 4572.
Zika Active Pregnancy Surveillance System (ZAPSS) in Puerto Rico Fact Sheet (English and Spanish)
Testing for Zika Virus
Language:
English
Recommend on FacebookTweet
Testing Information
What happens when I am tested for Zika and when will I get my results?
Only Some People Need Zika Testing
When to test for Zika Virus
Make sure to get your Zika test results
Zika Training for Healthcare Providers
Language:
English
Recommend on FacebookTweet
Zika Education
CDC Medical Epidemiologist Susan Hills, MBBS, MTH, presents an update on the epidemiologic and clinical aspects of the Zika outbreak. CDC Medical Officer Kiran Perkins, MD, MPH, also presents on the implications for pregnant women, including CDC’s updated interim clinical guidance.
During this meeting, pediatric health specialists, non-governmental partners, and federal officials gathered at CDC to discuss clinical evaluation and management of infants with congenital Zika virus infection in the United States. CDC considered discussions on clinical evaluation and management when developing interim guidance for healthcare providers.
Clinician Outreach and Communication Activity (COCA) Calls/Webinars
During COCA Calls/Webinars, subject matter experts present key emergency preparedness and response topics, followed by meaningful Q&A with participants. Each COCA Call/Webinar will offer the most up to date information and guidance for clinicians. Continuing Education is available for most calls/webinars.
A list of all published Zika-related reports. Continuing education is available for all MMWR reports.
Zika Virus: Information for Clinicians
Information for clinicians on Zika virus epidemiology, diagnoses and testing, case reporting, and clinical guidance and patient management.
CDC TRAIN provides free access to thousands of courses, more than 1,000 of which were developed by CDC programs and funded partners. Courses in CDC TRAIN are available on a wide array of public health and health care topics and in a variety of formats, including classroom training, webinars, and online self-study options. Many offer free continuing education. These links do not constitute an endorsement by Centers for Disease Control and Prevention (CDC). Only courses offered by CDC Course Providers have been verified and approved by CDC.
Patient Care
Dr. Joanne Cono, MD, ScM, Director of the Office of Science Quality of the CDC gave a live presentation regarding the latest Zika information available and answered a myriad of questions from your fellow health care practitioners.
Dr. Matt Karwowski, a pediatrician with the Pregnancy and Birth Defects Team for CDC’s 2016 Zika Virus Response, reviews what we know about Zika virus and congenital microcephaly and other birth defects. He also discusses CDC’s guidelines for healthcare providers caring for infants and children with possible Zika virus infection.
Dr. Titilope Oduyebo, an obstetrician-gynecologist from CDC’s Pregnancy and Birth Defects team, gives key insight into the Zika virus. She discusses what we know about Zika virus infection during pregnancy, and reviews CDC’s current recommendations for screening, testing, and management of women with possible Zika virus exposure.
Margaret Lampe, RN, MPH, a nurse scientist with the Pregnancy and Birth Defects Task Force for CDC’s 2016 Zika virus response shares an overview of the US Zika Pregnancy Registry and how to participate.
LABORATORY TRAINING RESOURCES
Training resources for laboratories .
For Laboratories
Language:
English
Recommend on FacebookTweet
In this Section
What’s New
New Lab Guidance
CDC, Division of Vector-Borne Diseases, Arboviral Diseases and Dengue Branches have updated diagnostic testing guidance for Zika, chikungunya, and dengue viruses.
More Resources
Resources and Publications
Language:
English
Recommend on FacebookTweet
Links to Zika Information Collections by Publisher
- Morbidity and Mortality Weekly Report (MMWR) Zika Reports
- Emerging Infectious Diseases (EID) Zika Spotlight
The conclusions, findings, and opinions expressed by authors contributing to EID do not necessarily reflect the official position of the U.S. Department of Health and Human Services (HHS), the Public Health Service (PHS), the Centers for Disease Control and Prevention (CDC), or the authors’ affiliated institutions. Use of trade names is for identification only and does not imply endorsement by PHS or by HHS.
- New England Journal of Medicine, Zika Virus Collection
- BMJ, Zika Virus
- Elsevier Zika Virus Resource Center
- Lancet Zika Virus Resource Centre
- Oxford University Press (including Journal of Infectious Diseases, Clinical Infectious Diseases, and American Journal of Tropical Medicine and Hygiene), Special Collection on Aedes aegypti and Zika Virus Research
- PLOS Collections, Zika
- John Wiley & Sons, Latest Zika Research
Emergency Bulletins
Links to U.S. and International Governmental Resources
Search the Biomedical Literature
PubMed, a service of the National Library of Medicine, includes over 15 million citations for biomedical articles back to the 1950’s. These citations are from MEDLINE and additional life science journals. PubMed includes links to many sites providing full text articles and other related resources.
Search Pub Med:
Notice: You are leaving the CDC website. We have provided a link to this site because it has information that may be of interest to you. CDC does not necessarily endorse the views or information presented on this site. Furthermore, CDC does not endorse any commercial products or information that may be presented or advertised on the site that is about to be displayed.
Communication Resources
Language:
English
Recommend on FacebookTweet
CDC offers free resources including video, fact sheets, and posters. Below are links to current communication tools and resources available for use and distribution. For information and resources for specific audiences, click the “Information for Specific Groups” tab in the navigation bar to the left.
Podcasts
Zika Update – This podcast series is designed to highlight the most important need to know information about Zika virus and its effects.
Zika Prevention: Do Your Part – This podcast series, available in English and Spanish, is a special novella series about Zika prevention and protection against mosquitoes.
Zika and Pregnancy: What Pregnant Women Need to Know – Learn more about what Zika is, what it means for pregnant women, and how you can protect your pregnancy..
Public Health Image Library (PHIL)
Public Health Image Library (PHIL) – The Public Health Image Library, or PHIL, was designed to share CDC public health images. CDC welcomes public health professionals, the media, laboratory scientists, educators, students, and the public to use this material for reference, teaching, presentations, and public health messages.
Press Information
The Zika Virus Digital Press Kit contains videos, photos, spokesperson biographies, releases, MMWR reports, and other relevant information for members of the media.
Vital Signs Issue: Zika and Pregnancy
Digital Resources
Widget
Blogs
- CDC Director Blog – Thoughts from CDC Director Tom Frieden, MD, MPH
- Public Health Matters – A collective blog about the exciting public health work of preventing and controlling infectious diseases that result from the interaction of people, animals, and the environment.
- NIOSH Science Blog – A scientific look at workplace safety and health issues from the National Institute for Occupational Safety and Health.
Social Media
Facebook
Twitter
Latest Tweets
With the right resources, we can develop better ways to combat the mosquito that spreads #Zika & other diseases.https://t.co/5KWn3rDG2z
Why the #Zika virus presents an unprecedented threat to the people of our nation, especially pregnant women. https://t.co/5KWn3rDG2z
Zika 101 Presentation
Zika Virus: Information for Clinicians
Zika Virus Microsite
Add real-time Zika virus information to your web site!
Images
Timeline of “What’s New”
Language:
English
Recommend on FacebookTweet
Keep up with CDC updates on Zika by signing up for email updates, subscribing to RSS, and syndicating available content about Zika. The Top 5 items are available for syndication.
- LGBT Community: How to protect yourselves from Zika[PDF – 2 pages]THURSDAY, SEPTEMBER 01, 2016
- UPDATE: Areas of Active Transmission for the Purpose of Blood and Tissue Safety InterventionTHURSDAY, SEPTEMBER 01, 2016
- Revised FDA Recommendations for Reducing the Risk of Zika Virus Transmission by Blood and Blood ComponentsSATURDAY, AUGUST 27, 2016
- Key Considerations for Healthcare Settings[PDF – 2 pages]TUESDAY, AUGUST 23, 2016
- When to Test for Zika Virus[PDF – 1 page]TUESDAY, AUGUST 23, 2016
- Zika Virus Testing for Any Pregnant Woman Not Living in an Area With Zika[PDF – 2 pages]TUESDAY, AUGUST 23, 2016
- HAN- CDC Expands Guidance for Zika Related to Mosquito-borne Transmission in Miami-Dade, FloridaMONDAY, AUGUST 22, 2016
- Update: Advice for People Living in or Traveling to South FloridaFRIDAY, AUGUST 19, 2016
- Support for Families of Newborns Affected by ZikaFRIDAY, AUGUST 19, 2016
- Resources and Guidance for Healthcare Providers Caring for Infants Affected by Zika VirusFRIDAY, AUGUST 19, 2016
- Collection and Submission of Specimens for Zika Virus Testing at Time of BirthFRIDAY, AUGUST 19, 2016
- Collection and Submission of Fetal Tissues for Zika Virus TestingFRIDAY, AUGUST 19, 2016
- UPDATE: Interim Guidance for the Evaluation and Management of Infants with Possible Congenital Zika Virus Infection – United States, August 2016FRIDAY, AUGUST 19, 2016
- UPDATE: Webcast Recordings for Clinical Evaluation & Management of Infants with Congenital Zika InfectionTHURSDAY, AUGUST 18, 2016
- Contraceptive Use Among Nonpregnant and Postpartum Women in the Context of Zika Preparedness – United StatesTUESDAY, AUGUST 02, 2016
- Contraception to Prevent Unintended Pregnancy during the Zika Virus OutbreakTUESDAY, AUGUST 02, 2016
- Update: Women & Their PartnersTUESDAY, AUGUST 02, 2016
- Press release: Travel guidance related to Miami neighborhoodMONDAY, AUGUST 01, 2016
- Zika is in Your Area: What to DoMONDAY, AUGUST 01, 2016
- Advice for people living in or traveling to Wynwood, a neighborhood in FloridaMONDAY, AUGUST 01, 2016
- Zika Community Action Response ToolkitMONDAY, AUGUST 01, 2016
- Updated: CDC Interim Zika Response Plan[PDF – 57 pages]SUNDAY, JULY 31, 2016
- Update: Ongoing Zika Virus Transmission – Puerto Rico, November 1, 2015-July 7, 2016SATURDAY, JULY 30, 2016
- Florida investigation links four recent Zika cases to local mosquito-borne virus transmissionFRIDAY, JULY 29, 2016
- FDA Statement: Advice to Blood Collection Establishments on Non-Travel Related Cases of Zika Virus in FloridaTHURSDAY, JULY 28, 2016
- Update: Interim Guidance for Health Care Providers Caring for Pregnant Women with Possible Zika Virus ExposureTUESDAY, JULY 26, 2016
- Update: Interim Guidance for Prevention of Sexual Transmission of Zika Virus – United States, July 2016TUESDAY, JULY 26, 2016
- New FDA Donor Screening Recommendations to Prevent Zika Transmisison[76 KB, 10 Pages]FRIDAY, JULY 22, 2016
- Zika: Protecting Camp Staff and Campers[682 KB, 2 Pages]WEDNESDAY, JULY 20, 2016
- Zika: Protecting Children from Mosquito Bites at Camp[539 KB, 2 Pages]WEDNESDAY, JULY 20, 2016
- CDC assisting Utah investigation of Zika virusTUESDAY, JULY 19, 2016
- Clinical Evaluation & Management of Infants with Congenital Zika InfectionTUESDAY, JULY 19, 2016
- Pregnancy Registry Factsheet for Tribal Healthcare Providers[752 KB, 2 Pages]THURSDAY, JULY 14, 2016
- Guidance for District and School AdministratorsTHURSDAY, JULY 14, 2016
- Country Classification Technical GuidanceWEDNESDAY, JULY 13, 2016
- “Prevención del zika: Colabore” Novella Podcast: Controle los mosquitos que están en el exterior (Spanish)TUESDAY, JULY 12, 2016
- Information on Aerial Spraying in Puerto RicoTUESDAY, JULY 12, 2016
- Zika Response & Success StoriesTUESDAY, JULY 12, 2016
- CDC Emergency Vector Control Request Form[47 KB]THURSDAY, JUNE 30, 2016
- CDC Zika Update Podcast: A Summary of the Outbreak 6/30/2016THURSDAY, JUNE 30, 2016
- Travel to Puerto Rico Flyer[2.5 MB, 1 Pages]MONDAY, JUNE 27, 2016
- Zika Virus: Information for Clinicians[6.6 MB, 56 Pages]THURSDAY, JUNE 23, 2016
- NIOSH Poster for Cruise Line Employees[187 KB, 1 Page]FRIDAY, JUNE 17, 2016
- NIOSH Fact Sheet for Cruise Line Employees[571 KB, 1 Page]FRIDAY, JUNE 17, 2016
- US Citizens Living in Areas with Zika TransmissionTHURSDAY, JUNE 16, 2016
- Travelers Visiting Friends and Family in Areas with Chikungunya, Dengue, or ZikaTHURSDAY, JUNE 16, 2016
- CDC Draft Interim Zika Response Plan[974 KB, 58 Pages]TUESDAY, JUNE 14, 2016
- Fact Sheet for Outdoor Activities[2.59 MB, 1 Page]MONDAY, JUNE 13, 2016
- ZAP Follow-Up Teleconference- Zika Diagnostic Tools, Testing, Algorithms, and Interpretations GuidanceMONDAY, JUNE 13, 2016
- ZAP Follow-Up Teleconference – Zika Surveillance in US StatesWEDNESDAY, JUNE 08, 2016
- “Zika Activity Book” For kids in the US[1.4 MB, 9 Pages]FRIDAY, JUNE 03, 2016
- MMWR Interpretation of Zika Virus Antibody Test ResultsFRIDAY, JUNE 03, 2016
- For Parents: A positive Zika virus test: What does it mean for my child?[439 KB, 2 Pages]THURSDAY, JUNE 02, 2016
- ZAP Follow-Up Teleconference – Pregnancy Planning in Areas with ZikaWEDNESDAY, JUNE 01, 2016
- ZAP Follow-Up Teleconference – Prevention of Sexually Transmitted ZikaWEDNESDAY, JUNE 01, 2016
- Zika Training ResourcesTUESDAY, MAY 31, 2016
- How to Protect Yourself Against Mosquito Bites (For Puerto Rico)[516 KB, 2 Pages]FRIDAY, MAY 27, 2016
- For Men: A Positive Zika Test- What Does it Mean for me?[393 KB, 2 Pages]FRIDAY, MAY 27, 2016
- Zika Active Pregnancy Surveillance System (ZAPSS) in Puerto Rico Fact Sheet (English and Spanish)[5.6 MB, 2 Pages]FRIDAY, MAY 27, 2016
- HAN: 389 Diagnostic Testing of Urine SpecimensWEDNESDAY, MAY 25, 2016
- Technical Statement on the Role of Disinsection in the Context of Zika OutbreaksTUESDAY, MAY 24, 2016
- MMWR Possible Zika Virus Infection Among Pregnant WomenFRIDAY, MAY 20, 2016
- Cases in Pregnant WomenFRIDAY, MAY 20, 2016
- Zika Active Pregnancy Surveillance SystemFRIDAY, MAY 20, 2016
- How to Protect Against Mosquito Bites[589 KB, 2 Pages]THURSDAY, MAY 19, 2016
- Zika: The Basics and How to Protect Against it[2 MB, 2 Pages]TUESDAY, MAY 17, 2016
- UPDATED Diagnostic TestingSUNDAY, MAY 15, 2016
- UPDATED Collection and Submission of Body FluidsSUNDAY, MAY 15, 2016
- MMWR: Comparison of Test Results for Zika Virus RNA in Urine, Serum, and Saliva SpecimensWEDNESDAY, MAY 11, 2016
- MMWR: Interim Guidance for Zika Virus Testing of UrineWEDNESDAY, MAY 11, 2016
- Zika and Sexual Transmission: What we know and what we don’t know[2.8 MB, 1 Page]TUESDAY, MAY 10, 2016
- How Zika Spreads[5.4 MB, 1 Page]MONDAY, MAY 09, 2016
- Prevention: Controlling Mosquitoes at HomeFRIDAY, APRIL 29, 2016
- Zika Activity Book: For kids in areas with Zika[1.4 MB, 9 Pages]FRIDAY, APRIL 29, 2016
- HIV Infection and Zika VirusTUESDAY, APRIL 26, 2016
- Interim Guidance for Protecting Workers from Occupational Exposure to Zika Virus[475 KB, 7 Pages]FRIDAY, APRIL 22, 2016
- US Zika Pregnancy Registry: What Parents Need to Know[1.6 MB, 1 Page]FRIDAY, APRIL 22, 2016
- Male-to-Male Sexual Transmission of Zika Virus – Texas, January 2016FRIDAY, APRIL 15, 2016
- Survey of Blood Collection Centers and Implementation of Guidance for Prevention of Transfusion-Transmitted Zika Virus Infection – Puerto Rico, 2016FRIDAY, APRIL 15, 2016
- Vital Signs: Preparing for Local Mosquito-Borne Transmission of Zika Virus – United States, 2016FRIDAY, APRIL 08, 2016
- Doctor’s visit checklist: For Pregnant Women who Travel to an area with Zika[1.7 MB, 2 Pages]FRIDAY, APRIL 01, 2016
- Zika Action Plan SummitFRIDAY, APRIL 01, 2016
- Doctor’s visit checklist: For Pregnant Women Living in an Area with Zika[1.7 MB, 2 Pages]FRIDAY, APRIL 01, 2016
- Zika Virus Testing for Pregnant Women Living in an Area with Zika (fact sheet)[1.7 MB, 2 Pages]FRIDAY, APRIL 01, 2016
- For Pregnant Women: A Positive Zika Virus Test, What Does it Mean for me? (fact sheet)[237 KB, 1 Page]FRIDAY, APRIL 01, 2016
- Congenital Microcephaly Case DefinitionsTHURSDAY, MARCH 31, 2016
- Preconception counseling guide for men and women living in areas with ZikaSATURDAY, MARCH 26, 2016
- UPDATE: QA: Pregnant Women and Women of Reproductive AgeSATURDAY, MARCH 26, 2016
- Women and their partners who are thinking about pregnancySATURDAY, MARCH 26, 2016
- MMWR: UPDATE Interim Guidance for Prevention of Sexual Transmission of Zika Virus – United States, 2016FRIDAY, MARCH 25, 2016
- MMWR: UPDATE: Interim Guidance for Health Care Providers Caring for Women of Reproductive Age with Possible Zika Virus Exposure – United States, 2016FRIDAY, MARCH 25, 2016
- MMWR: Estimating Contraceptive Needs and Increasing Access to Contraception in Response to the Zika Virus Disease Outbreak – Puerto Rico, 2016FRIDAY, MARCH 25, 2016
- Zika Communication Planning Guide for StatesMONDAY, MARCH 21, 2016
- Tools for Health Care ProvidersMONDAY, MARCH 21, 2016
- US Zika Pregnancy RegistryMONDAY, MARCH 21, 2016
- Information for ParentsSUNDAY, MARCH 20, 2016
- Interim CDC Recommendations for Zika Vector Control in the Continental United StatesFRIDAY, MARCH 18, 2016
- Biosafety Guidance for Transportation of Specimens and for Work with Zika Virus in the LaboratoryWEDNESDAY, MARCH 16, 2016
- College Spring Break fact sheet[2.2 MB, 1 Page]WEDNESDAY, MARCH 16, 2016
- Family Spring Break fact sheet[2.2 MB, 1 Page]WEDNESDAY, MARCH 16, 2016
- Zika and Sex: Information for men with pregnant partners living in areas with Zika fact sheet[1.8 MB, 1 Page]WEDNESDAY, MARCH 16, 2016
- Zika and Sex: Information for pregnant women living in areas with Zika fact sheet[1.6 MB, 1 Page]WEDNESDAY, MARCH 16, 2016
- For pregnant women in areas with Zika: Protect your pregnancy fact sheet[1.6 MB, 1 PageWEDNESDAY, MARCH 16, 2016
- Zika Virus Risk-Based Preparedness and Response Guidance for StatesWEDNESDAY, MARCH 09, 2016
- MMWR: Increase in Reported Prevalence of Microcephaly in Infants Born to Women Living in Areas with Confirmed Zika Virus Transmission During the First Trimester of Pregnancy – Brazil, 2015TUESDAY, MARCH 08, 2016
- Top 10 Zika Response Planning Tips: Brief Information for State, Tribal, and Territorial Health OfficialsFRIDAY, MARCH 04, 2016
- Build your own Zika prevention kitTHURSDAY, MARCH 03, 2016
- MMWR: Transmission of Zika Virus Through Sexual Contact with Travelers to Areas of Ongoing Transmission – Continental United States, 2016SUNDAY, FEBRUARY 28, 2016
- MMWR: Zika Virus Infection Among U.S. Pregnant Travelers – August 2015-February 2016SUNDAY, FEBRUARY 28, 2016
- Zika MAC-ELISA Emergency Use AuthorizationSUNDAY, FEBRUARY 28, 2016
- Collection and Submission of Body Fluids for Zika Virus TestingFRIDAY, FEBRUARY 26, 2016
- Update: Interim Guidelines for Prevention of Sexual Transmission of Zika Virus – United States, 2016WEDNESDAY, FEBRUARY 24, 2016
- Update: Interim Guidelines for Healthcare Providers Caring for Infants and Children with Possible Zika Virus Infection – United States, February 2016SATURDAY, FEBRUARY 20, 2016
- QA: Healthcare Providers Caring for Infants and Children with Possible Zika Virus InfectionSATURDAY, FEBRUARY 20, 2016
- Pregnant? Read this before you travel[3.4 MB, 2 Pages]THURSDAY, FEBRUARY 18, 2016
- Zika: What we know and what we don’t know[4.4 MB, 1 Page]THURSDAY, FEBRUARY 18, 2016
- Pregnant and living in an area with Zika?[2.1 MB, 2 Pages]WEDNESDAY, FEBRUARY 17, 2016
- Pregnant? Read this before you travel[3.4 MB, 1 Page]SATURDAY, FEBRUARY 13, 2016
- Fetal Tissue Collection and SubmissionFRIDAY, FEBRUARY 12, 2016
- Interim Guidelines for Prevention of Sexual Transmission of Zika Virus – United States, 2016FRIDAY, FEBRUARY 12, 2016
- Zika Virus Disease Q&AFRIDAY, FEBRUARY 12, 2016
- Travelers’ Health: Practice enhanced precautionsTHURSDAY, FEBRUARY 11, 2016
- Questions and Answers for Healthcare Providers Caring for Pregnant Women and Women of Reproductive Age with Possible Zika Virus ExposureTUESDAY, FEBRUARY 09, 2016
- QA: Guillain-Barre SyndromeMONDAY, FEBRUARY 08, 2016
- Revised diagnostic testing for Zika, chikungunya, and dengue viruses in US Public Health Laboratories[973 KB, 6 Pages]SUNDAY, FEBRUARY 07, 2016
- QA: Zika and Sexual TransmissionFRIDAY, FEBRUARY 05, 2016
- Zika and PregnancySATURDAY, JANUARY 30, 2016
- Interim Guidelines for the Evaluation and Testing of Infants with Possible Congenital Zika Virus Infection – United States, 2016THURSDAY, JANUARY 28, 2016
- Questions and Answers for Pediatric Healthcare Providers: Infants and Zika Virus InfectionTUESDAY, JANUARY 26, 2016
- Surveillance and Control of Aedes aegypti and Aedes albopictus in the United StatesMONDAY, JANUARY 25, 2016
- Interim Guidelines for Pregnant Women During a Zika Virus OutbreakTHURSDAY, JANUARY 21, 2016
- CDC Health Alert Network advisory for Zika virusFRIDAY, JANUARY 15, 2016
Zika Virus Response Planning: Interim Guidance for District and School Administrators in the Continental United States and Hawaii
Language:
English
Recommend on FacebookTweet
Summary
What is already known about this topic?
Zika virus is transmitted primarily through the bite of infected Aedes species mosquitoes. Zika virus is not transmitted directly from one person to another through casual contact. There is no evidence that risk for transmission on school properties will be higher than in other areas of the local community.
What is added by this report?
If suspected or confirmed Zika virus infection occurs in a student or staff member, schools should continue to prioritize strategies to prevent mosquito bites on school grounds, to prevent further transmission through infected mosquitoes. Because Zika virus is not transmitted from person to person by casual contact, it is not necessary to issue a schoolwide notification, and students or staff members with travel-related Zika virus exposure or confirmed Zika virus infection do not need to be removed from school. Isolation of persons with Zika virus disease or quarantine of exposed persons is neither recommended nor appropriate. Schools should maintain privacy and nondiscrimination protections for all students and employees. In the case of local Zika virus transmission, it is not necessary to cancel school-related activities.
What are the implications for public health practice?
School, local, and public health authorities should work together to implement mosquito control activities and mosquito bite prevention measures in schools to decrease risk of Zika virus transmission, to apply appropriate policies for educating students and staff members, and for continuation of school operations.
CDC has developed interim guidance for kindergarten through grade 12 (K–12) district and school administrators for public health actions pertaining to Zika virus infection. This guidance is intended to address concerns about the risk for Zika virus infection in K–12 schools in the continental United States and Hawaii, provide school districts with information for planning school-related activities, and recommend actions that can be taken, in consultation with local public health authorities and government officials, to reduce the potential risk for Zika virus transmission on school premises and among students. This guidance provides an overview of the potential roles and responsibilities of public health authorities and school officials, describes prevention measures that schools can take to reduce mosquito exposure, and provides information on responding to a case of travel-associated Zika virus infection or confirmed local mosquito-borne transmission of Zika virus (See Key Points). Considerations for child care, camp, and higher education settings also are addressed. This guidance will be updated as needed when new information becomes available. The latest available Zika virus information, including answers to commonly asked questions, can be found online. Related relevant resources are summarized in Additional Resources below.
General Information about Zika Virus
Since 2007, Zika virus disease outbreaks have been reported in the South Pacific, and since 2015, Zika virus has rapidly spread in the Western Hemisphere.1,2 Zika virus is transmitted primarily through the bite of infected Aedes species mosquitoes.3 Mosquitoes become infected when they consume blood from a person infected with the virus. Infected mosquitoes can then spread the virus to other persons through bites. Direct human-to-human transmission of Zika virus can occur through sexual contact and from a pregnant woman to her fetus.4,5 Zika virus infection during pregnancy can cause severe birth defects, including microcephaly.5 Zika virus is not transmitted directly from one person to another through casual contact.
The signs and symptoms of Zika virus infection in children are similar to those in adults.6 Most persons infected with Zika virus will not have symptoms; among those who do become ill, the most common signs and symptoms are fever, rash, joint pain, and conjunctivitis, and these usually occur within a week of infection.6 The illness is typically mild, with symptoms lasting for several days to a week. Most children and adults infected with Zika virus do not become ill enough to seek medical care or require hospitalization, and death from Zika virus infection is rare. Cases of Guillain-Barré syndrome, a rare autoimmune condition manifested by muscle weakness (occasionally leading to temporary paralysis), have been reported among persons who have had Zika virus infection. 7 It is not known how often Guillain-Barré syndrome has occurred in children after Zika virus infection. There is currently no vaccine or specific drug to prevent or treat Zika virus infection.
Zika virus infection in childhood has not currently been linked to developmental delays or impaired growth. Because symptoms of Zika virus disease are similar to symptoms of other viral infections that commonly occur among school children, as well as less common infections such as measles, it is important that educators remain vigilant in recognizing signs and symptoms of more easily transmissible infections while planning specific interventions related to Zika virus disease.
Local mosquito-borne Zika virus transmission has been reported in the continental United States. However, there is no evidence that risk for transmission on school properties will be higher than in other areas of the local community
Roles and Responsibilities of School Officials and Public Health Authorities
Public health authorities play a pivotal role in identifying the risk for Zika virus exposure in different settings and providing advice on actions to reduce the risk. Schools, functioning both as educational settings and as employers, have a critical role in sharing information from public health authorities, as well as in addressing concerns and questions raised by students, families, and staff members about Zika virus, and implementing public health authorities’ recommendations for schools in a timely fashion. School administrators should understand the roles and responsibilities of public health authorities and consult with them regarding questions or issues related to Zika virus infection.
Public health authorities and school districts should proactively and collaboratively establish direct communication channels and clearly define each partner’s roles and responsibilities. Initial efforts should include identifying points of contact for communication and developing protocols for implementing public health recommendations. School authorities, working collaboratively with local public health authorities, should review and ensure compliance with public health codes and applicable Occupational Safety and Health Administration (OSHA) standards, including OSHA guidance for protecting workers from occupational exposure to Zika virus.10 OSHA recommends that employers provide insect repellents for outdoor workers and consider modifying work responsibilities, if requested by the employee, of women who are pregnant or who might become pregnant, and men who have a sexual partner who is pregnant or might become pregnant.10
Planning for Possible Zika Virus Transmission in K–12 Schools
Outside of their homes, children and adolescents spend much of their time at school. Accordingly, district and school administrators play an important role in efforts to prevent possible Zika virus transmission among students and their families, particularly in schools that open their facilities to the community for events, extracurricular programs, and recreational use.
Prevention of mosquito bites through an integrated vector management plan is of paramount importance for avoiding Zika virus infections.11 Schools can help to reduce risk for students, families, and the community by implementing mosquito control measures on school grounds, such as identifying and removing sources of standing water that can serve as mosquito breeding sites. Common sources on school grounds can include buckets, trash cans, planters, tires, tall grasses, playground equipment, and spaces beneath temporary modular structures. Adjustments can be made to ensure these do not become mosquito breeding areas, including regularly cleaning, turning over, tightly covering, or completely removing (if appropriate) these sources; sweeping away pools of water; and keeping all grassy areas mowed (including less-traveled and hard-to-access areas such as under bleachers). In addition, efforts should be made to prevent mosquitoes from entering classrooms by placing new screens or replacing damaged screens in windows and doors, or by using air conditioning when available.
The use of other methods of mosquito control in a school or community, including insecticide spraying, is decided upon by the local and state jurisdictions. The public health and school partnership can work with local government officials to learn which approaches are available and appropriate to prevent transmission of Zika and other mosquito-borne viruses, such as West Nile, dengue, and chikungunya.12 If presence of mosquitoes at a school appears to remain high despite taking recommended steps, including removing sources of standing water, this might indicate unrecognized breeding sites, which can be a considerable source of mosquitoes. Local mosquito control authorities or licensed pest control contractors should be contacted to facilitate remediation.
When possible, students, staff members, and family members participating in outdoor activities in areas with mosquito activity should be advised to follow CDC Zika virus prevention guidelines, including wearing long pants and sleeves and using U.S. Environmental Protection Agency–registered insect repellents, all of which are considered safe for school-aged children and pregnant women.13,14 Schools should review and, if necessary, update their policies regarding student possession and application of insect repellent, and inform students, their caregivers, and staff members of updated plans or policies. Administrators might also need to consider logistical issues involved, including purchasing responsibilities for repellents and the processes for applying them to large groups of children when necessary. Schools should consider risk for potential exposure to mosquito-borne diseases when planning field trips and other school-sponsored travel. Although the mosquitoes that transmit Zika virus are more active during the day, they can bite and spread infection at any time.13 If travel outside the continental United States and Hawaii is planned, risk for exposure to Zika virus might exist. CDC’s Travel Information website includes information about the current Zika virus situation in specific countries.15
Zika virus can also be transmitted sexually.4 Nationwide, 41% of high school–aged students report having had sexual intercourse at least once.16Therefore, age-appropriate sexual health education should include information regarding the risk for Zika virus during pregnancy and the potential for sexual transmission of Zika virus, including that correct and consistent condom use can reduce the likelihood of sexual transmission of Zika virus, other sexually transmitted infections, and unintentional pregnancy, and that abstinence can eliminate these risks.4,17
Responding to a Case of Zika Virus Infection in K–12 Schools
While planning for possible cases of Zika virus infection in schools, educators should maintain provision of a safe, consistent, and effective learning environment. If a case of Zika virus infection is suspected or confirmed in a student or staff member, schools should continue to prioritize strategies to prevent mosquito bites on school grounds, to prevent further transmission through infected mosquitoes. Administrators, educators, and school health professionals can disseminate accurate Zika virus information to students and families, and prevent stigma related to perception of a student’s risk for Zika virus through efforts such as dispelling of myths and ensuring no particular students or groups are targeted for social exclusion.
In the event of a case of Zika virus disease in a student or staff member at a K–12 school, medical privacy and confidentiality should be maintained. Because Zika virus is not transmitted from person to person by casual contact, it is not necessary to issue a schoolwide notification, and students or staff members with travel-related Zika virus exposure or confirmed Zika virus infection do not need to be removed from school. Isolation of persons with Zika virus disease or quarantine of exposed persons is neither recommended nor appropriate. Patients with symptomatic illness should receive appropriate supportive medical management.
Children with fever or symptoms that might be associated with Zika virus infection, including rash, conjunctivitis, or joint pain, should be managed according to school illness policies, regardless of potential for Zika virus infection.18 School nurses and other staff members should continue to adhere to OSHA bloodborne pathogen standard precautions for any potential body fluid contact in the course of their duties.19
Responding to Mosquito-Borne Transmission of Zika Virus in the Local Area
If local mosquito-borne transmission of Zika virus occurs, state and local jurisdictions and public health authorities will inform school districts of the range of the affected areas, provide recommendations based on cases reported in the local community, and guide schools and school districts in the implementation of enhanced measures, if required.12 This might include providing options, if requested by the employee, to limit outdoor duties or activities of students and staff members who are pregnant, who might be pregnant, or who are trying to conceive. While implementing these measures, schools should continue to maintain privacy and nondiscrimination protections for all students and employees. Zika virus testing might be offered by health authorities for pregnant staff members and students, and for persons exhibiting symptoms consistent with Zika virus disease.20
School administrators, in close coordination with local officials, will need to consider local factors, such as climate, landscape of school grounds and their surroundings, and proximity of Zika virus transmission to the school, to determine what additional measures to undertake.12 It is not necessary to suspend or cancel classes (including physical education classes), outdoor recess or outdoor activities, outdoor sporting events, or extracurricular activities.
Considerations for Child Care, Camp, and Higher Education Settings
In addition to schools, locations where children and adolescents routinely gather, such as child care facilities, camps (including day camps and overnight camps), and institutions of higher education (colleges and universities), should also consider strategies for preventing Zika virus transmission. In these settings, interventions to prevent and prepare for Zika virus infection should, at minimum, be consistent with the recommendations for K–12 schools. Administrators should act in accordance with regulations concerning public health issues relevant to their specific settings. The Administration for Children and Families has developed informational resources for child care providers to prepare for Zika virus21, and CDC has developed Zika virus communication toolkits for day camp and overnight camp settings, as well as for colleges and universities.22 College and university administrators should pay particular attention to issues relevant to students in this age group, including sexual transmission, guidance for pregnant women and their male sexual partners, and travel advisories.
Key Points
- Zika virus is spread primarily through the bite of an infected Aedes species mosquito, through sexual contact, or from a pregnant woman to her fetus. Zika virus is not passed directly from person to person through casual contact.
- For most children and adults, Zika virus infection will not cause symptoms or will only cause mild symptoms.
- Zika virus infection during pregnancy is associated with adverse pregnancy outcomes and certain birth defects; therefore, special considerations for preventing exposure might be needed for pregnant women, women trying to conceive, and their male sexual partners.
- School jurisdictions should proactively establish effective channels of communication with local government and public health authorities regarding response plans for local transmission of Zika virus disease.
- School administrators can help provide safe school environments through mosquito bite prevention efforts and sharing of accurate Zika virus information with staff members, students, and families.
- It is not recommended for schools to remove students or staff members who have Zika virus disease or who were exposed to Zika virus, or to cancel school-related activities because of Zika virus concerns.
- Nondiscrimination and privacy and confidentiality measures should be maintained for all students and staff members.
Authors
Eric J. Dziuban, MD, Division of Human Development and Disability, National Center on Birth Defects and Developmental Disabilities, CDC; Jessica L. Franks, MPH, Division of Human Development and Disability, National Center on Birth Defects and Developmental Disabilities, CDC; Marvin So, MPH, Division of Human Development and Disability, National Center on Birth Defects and Developmental Disabilities, CDC; Aron J. Hall, DVM, Division of Viral Diseases, National Center for Immunization and Respiratory Diseases, CDC; Heather J. Menzies, MD, Division of Global Health Protection, Center for Global Health, CDC; Susan L. Hills, MBBS, Division of Vector-Borne Diseases, National Center for Emerging and Zoonotic Infectious Diseases, CDC; Marc Fischer, MD, Division of Vector-Borne Diseases, National Center for Emerging and Zoonotic Infectious Diseases, CDC
Acknowledgments
American Academy of Pediatrics, Elk Grove Village, Illinois (Committee on Pediatric Emergency Medicine, Council on Environmental Health, Council on School Health, Disaster Preparedness Advisory Council); Association of State and Territorial Health Officials, Arlington, Virginia; National Association of County and City Health Officials, Washington, D.C.; National Association of School Nurses, Silver Spring, Maryland; American Federation of Teachers, Washington, D.C.; Administration for Children and Families, U.S. Department of Health and Human Services, Washington, D.C.; Amra Uzicanin, MD, Division of Global Migration and Quarantine, CDC; Lisa Barrios, DrPH, Division of Adolescent and School Health, CDC; Georgina Peacock, MD, Division of Human Development and Disability, CDC.
Corresponding author: Eric J. Dziuban, edziuban@…, 404-718-8394.
References
- Duffy MR, Chen TH, Hancock WT, et al. Zika virus outbreak on Yap Island, Federated States of Micronesia. N Engl J Med 2009;360:2536–43.
- CDC. Zika virus: Areas with Zika. Atlanta, GA: US Department of Health and Human Services, CDC; 2016.
- CDC. Zika virus: About estimated range of Aedes aegypti and Aedes albopictus in the United States, 2016 Maps. Atlanta, GA: US Department of Health and Human Services, CDC; 2016.
- Oster AM, Russell K, Stryker JE, et al. Update: Interim guidance for prevention of sexual transmission of Zika virus—United States, 2016.MMWR Morb Mortal Wkly Rep 2016;65:323–5.
- Rasmussen SA, Jamieson DJ, Honein MA, Petersen LR. Zika virus and birth defects—reviewing the evidence for causality. N Engl J Med2016;374:1981–7.
- CDC. Zika virus: What parents should know about Zika. Atlanta, GA: US Department of Health and Human Services, CDC; 2016.
- Cao-Lormeau VM, Blake A, Mons S, et al. Guillain-Barré syndrome outbreak associated with Zika virus infection in French Polynesia: a case-control study. Lancet 2016;387:1531–9.
- CDC. Zika virus disease in the United States, 2015–2016. Atlanta, GA: US Department of Health and Human Services, CDC; 2016.
- Hahn MB, Eisen RJ, Eisen L, et al. Reported distribution of Aedes (Stegomyia) aegypti and Aedes (Stegomyia) albopictus in the United States, 1995–2016 (Diptera: Culicidae). J Med Entomol 2016. Epub June 9, 2016.
- Occupational Safety and Health Administration. Interim guidance for protecting workers from occupational exposure to Zika virus. Washington, DC: US Department of Labor, Occupational Safety and Health Administration; 2016.
- CDC. Controlling mosquitoes at home. Atlanta, GA. US Department of Health and Human Services, CDC; 2016.
- CDC. Draft interim CDC Zika response plan (CONUS and Hawaii): Initial response to Zika virus. Atlanta, GA: US Department of Health and Human Services, CDC; 2016.
- CDC. Zika virus: Prevention. Atlanta, GA. US Department of Health and Human Services, CDC; 2016.
- US Environmental Protection Agency. Find the insect repellent that is right for you. Washington, DC: US Environmental Protection Agency; 2016.
- CDC. Zika travel information. Atlanta, GA. US Department of Health and Human Services, CDC; 2016.
- Kann L, McManus T, Harris WA, et al. Youth risk behavior surveillance—United States, 2015. MMWR Surveill Summ 2016;65(No. SS-6).
- CDC. Zika virus: Pregnant women: how to protect yourself. Atlanta, GA. US Department of Health and Human Services, CDC; 2016.
- Aronson SS, Shope T, editors. Managing infectious diseases in child care and schools. 3rd ed. Chicago, IL: American Academy of Pediatrics; 2013.
- Occupational Safety and Health Administration. Bloodborne pathogens and needlestick prevention. Washington, DC: US Department of Labor, Occupational Safety and Health Administration; 2016.
- Oduyebo T, Petersen EE, Rasmussen SA, et al. Update: interim guidelines for health care providers caring for pregnant women and women of reproductive age with possible Zika virus exposure—United States, 2016. MMWR Morb Mortal Wkly Rep 2016;65:122–7.
- Administration for Children and Families. Zika virus resources. Washington, DC: US Department of Health and Human Services, Administration for Children and Families; 2016.
- CDC. Zika communication toolkits. Atlanta, GA. US Department of Health and Human Services, CDC; 2016.
Additional Resources
Women Trying to Become Pregnant
Language:
English
Recommend on FacebookTweet
How to protect yourself
CDC recommends special precautions for women and their partners thinking about pregnancy.
What to do if you live in or travel to an area with Zika
If you aren’t pregnant, but you’re thinking about having a baby, here’s what you can do
Talk with your doctor or other healthcare provider
Women and their partners who are thinking about pregnancy should talk with their doctor or healthcare provider about
- Their plans for having children
- The potential risk of getting Zika during pregnancy
- Their partner’s potential exposures to Zika
The table below shows the suggested timeframes for waiting to get pregnant after possible exposure to Zika:
Suggested timeframe to wait before trying to get pregnant
|
| Possible exposure via recent travel or sex without a condom with a man infected with Zika |
|
Women |
Men |
| Zika symptoms |
Wait at least 8 weeks after symptoms start |
Wait at least 6 months after symptoms start |
| No Zika symptoms |
Wait at least 8 weeks after exposure |
Wait at least 8 weeks after exposure.
Talk with your healthcare provider |
| People living in areas with Zika |
|
Women |
Men |
| Zika symptoms |
Wait at least 8 weeks after symptoms start |
Wait at least 6 months after symptoms start |
| No Zika symptoms |
Talk with doctor or healthcare provider |
Talk with doctor or healthcare provider |
Decisions about pregnancy planning are personal and complex, and the circumstances for women and their partners will vary. Women and their partners should discuss pregnancy planning with a trusted doctor or healthcare provider. As part of counseling with healthcare providers, some women and their partners living in areas with active Zika virus transmission might decide to delay pregnancy.
PREVENTING PREGNANCY
If you decide that now is not the right time to have a baby, talk to your doctor or other healthcare provider.
Related Resources
For Women in Areas with Zika: Plan Your Pregnancy
Factsheets & posters
Learn more about Zika with our fact sheet
Resources and Publications
Language:
English
Recommend on FacebookTweet
Links to Zika Information Collections by Publisher
- Morbidity and Mortality Weekly Report (MMWR) Zika Reports
- Emerging Infectious Diseases (EID) Zika Spotlight
The conclusions, findings, and opinions expressed by authors contributing to EID do not necessarily reflect the official position of the U.S. Department of Health and Human Services (HHS), the Public Health Service (PHS), the Centers for Disease Control and Prevention (CDC), or the authors’ affiliated institutions. Use of trade names is for identification only and does not imply endorsement by PHS or by HHS.
- New England Journal of Medicine, Zika Virus Collection
- BMJ, Zika Virus
- Elsevier Zika Virus Resource Center
- Lancet Zika Virus Resource Centre
- Oxford University Press (including Journal of Infectious Diseases, Clinical Infectious Diseases, and American Journal of Tropical Medicine and Hygiene), Special Collection on Aedes aegypti and Zika Virus Research
- PLOS Collections, Zika
- John Wiley & Sons, Latest Zika Research
Emergency Bulletins
Links to U.S. and International Governmental Resources
Search the Biomedical Literature
PubMed, a service of the National Library of Medicine, includes over 15 million citations for biomedical articles back to the 1950’s. These citations are from MEDLINE and additional life science journals. PubMed includes links to many sites providing full text articles and other related resources.
Search Pub Med:
Notice: You are leaving the CDC website. We have provided a link to this site because it has information that may be of interest to you. CDC does not necessarily endorse the views or information presented on this site. Furthermore, CDC does not endorse any commercial products or information that may be presented or advertised on the site that is about to be displayed.
Morbidity and Mortality Weekly Report (MMWR)
http://www.cdc.gov/mmwr/zika_reports.html
MMWR Zika Reports
Language:
English
Recommend on FacebookTweet
September 2, 2016
August 26, 2016
August 5, 2016
July 29, 2016
July 22, 2016
June 24, 2016
June 3, 2016
May 27, 2016
May 13, 2016
May 6, 2016
April 22, 2016
April 15, 2016
April 8, 2016
April 1, 2016
March 25, 2016
March 18, 2016
March 11, 2016
March 4, 2016
February 26, 2016
February 19, 2016
February 12, 2016
January 29, 2016
January 22, 2016
.
.
WEBBIB1617
http://tinyurl.com/gtdzaq3
.
.
Sincerely,
David Dillard
Temple University
(215) 204 – 4584
jwne@…
http://workface.com/e/daviddillard
NET-GOLD
http://groups.yahoo.com/group/net-gold
http://listserv.temple.edu/archives/net-gold.html
https://groups.io/org/groupsio/net-gold/archives
http://net-gold.3172864.n2.nabble.com/
Research Guides
https://sites.google.com/site/researchguidesonsites/
Research Paper Writing
http://guides.temple.edu/research-papers
Employment
http://guides.temple.edu/employment-guide
Internships
http://guides.temple.edu/employment-internships
Hospitality
http://guides.temple.edu/hospitality-guide
Disabilities And Employment
http://guides.temple.edu/c.php?g=134557
Indoor Gardening
https://groups.yahoo.com/neo/groups/indoorgardeningurban/info
Educator-Gold
http://groups.yahoo.com/group/educator-gold/
K12ADMINLIFE
http://groups.yahoo.com/group/k12adminlife/
Public Health Resources Including Ebola
http://guides.temple.edu/public-health-guide
Blog
https://educatorgold.wordpress.com/
The Russell Conwell Learning Center Research Guide:
Information Literacy
http://tinyurl.com/78a4shn
Nina Dillard’s Photographs On Net-Gold
http://www.flickr.com/photos/neemers/
Twitter: davidpdillard
Temple University Site Map
https://sites.google.com/site/templeunivsitemap/home
Bushell, R. & Sheldon, P. (Eds),
Wellness and Tourism: Mind, Body, Spirit,
Place, New York: Cognizant Communication Books.
Wellness Tourism: Bibliographic and Webliographic Essay
David P. Dillard
http://tinyurl.com/p63whl
Railtram Discussion Group
from the union pacific to britrail and beyond
https://groups.yahoo.com/neo/groups/railtram/info
Indoor Gardening
improve your chances for indoor gardening success
http://tech.groups.yahoo.com/group/indoorgardeningurban/
Sport-Med
https://www.jiscmail.ac.uk/lists/sport-med.html
http://groups.yahoo.com/group/sports-med/
http://listserv.temple.edu/archives/sport-med.html
Health Diet Fitness Recreation Sports Tourism
https://groups.yahoo.com/neo/groups/healthrecsport/info
http://listserv.temple.edu/archives/health-recreation-sports-tourism.html
.
.
Please Ignore All Links to JIGLU
in search results for Net-Gold and related lists.
The Net-Gold relationship with JIGLU has
been terminated by JIGLU and these are dead links.
http://groups.yahoo.com/group/Net-Gold/message/30664
http://health.groups.yahoo.com/group/healthrecsport/message/145
Temple University Listserv Alert :
Years 2009 and 2010 Eliminated from Archives
https://sites.google.com/site/templeuniversitylistservalert/




















































 * Insect repellent brand names are provided for your information only. The Centers for Disease Control and Prevention and the U.S. Department of Health and Human Services cannot recommend or endorse any name brand products.
* Insect repellent brand names are provided for your information only. The Centers for Disease Control and Prevention and the U.S. Department of Health and Human Services cannot recommend or endorse any name brand products.













































































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
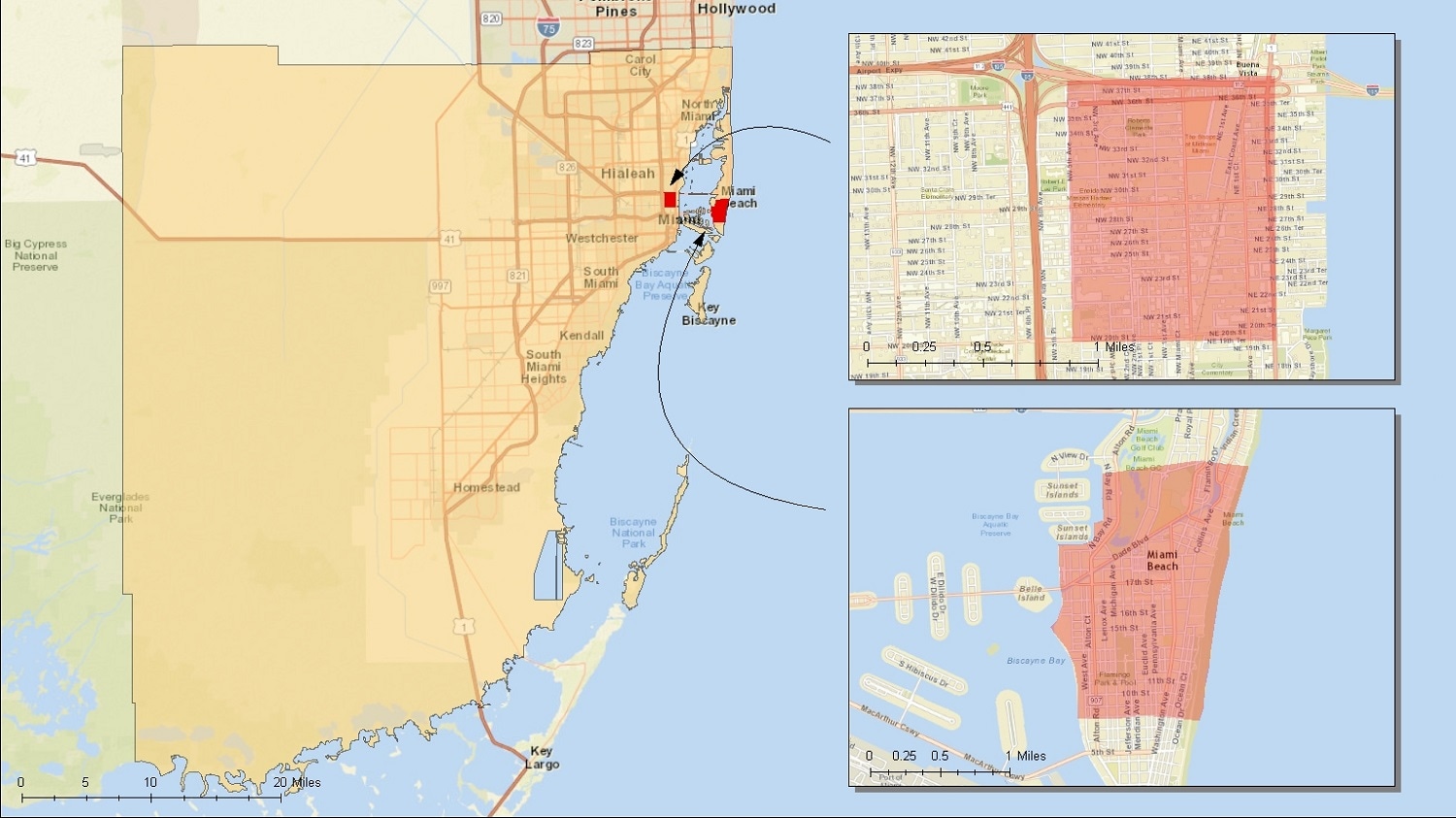{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
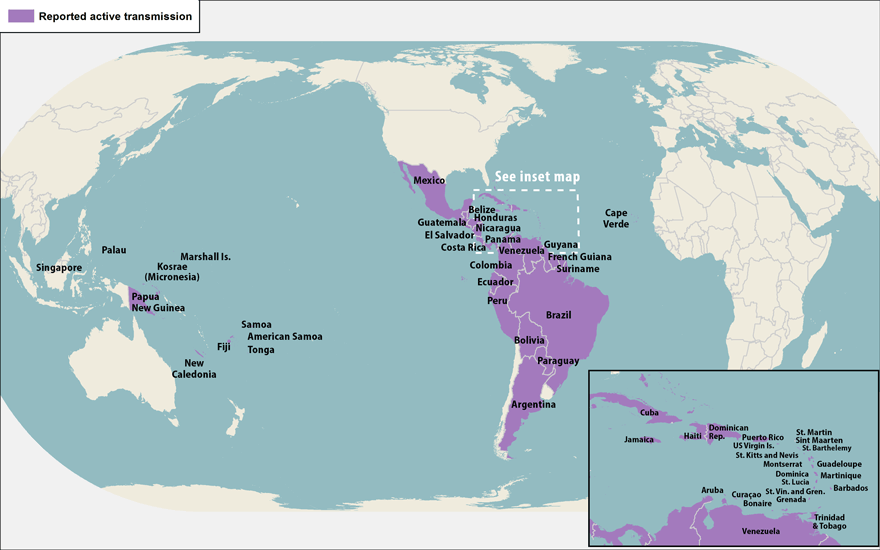{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}